
Open bone fractures—limb salvage or amputation? Putting ourselves in the position of the patient
BY IAIN MCFADYEN AND SAMIR MEHTA
In recent years, medical science has made significant advancements in treating major trauma cases, especially those involving extensive bone loss. We have witnessed remarkable progress in the field. However, it is crucial to recognize the human aspect of dealing with these challenging injuries and the importance of involving other healthcare professionals and the patient's family in the decision-making around limb salvage or amputation.
The medical world has developed amazing new techniques and technologies for coping with serious open extremity fractures. But sometimes we get caught up in the new techniques and what is possible surgically, so much so that might lose sight of what the patient goes through during the process of us trying to save their limbs.
When we talk about serious open fractures with bone loss, we’re really talking about dramatic cases with substantial amount of bone missing. There was a time not so long ago that, with injuries such as these, limb salvage was not an option and the conversation with the patient focused on amputation.
When these patients showed up in the emergency room, trauma or re-animation bay, there would be a lot of excitement around them—people would get their phones out and take pictures of the injuries—and we had less developed systems to assess the limb before eventually deciding it's not salvageable. The surgeon would simply decide it was not re-constructible and that amputation was the only option. Life before limb, always.
Today, we have better options to save limbs with more sophisticated tools in our armory—external fixators, intermediary nails that can lengthen and shorten, rings, ands screws and plates that have sensors. We can insert biology and we can move bone with its blood supply. Thanks to the work of our colleagues in plastic surgery, we do much better also with wound management.
Limb salvage with distraction osteogenesis or amputation?
While surgeons now have more options for limb salvage, it's essential to consider whether saving the limb is always the best solution. The dilemma lies in balancing the desire to preserve the limb with the patient's overall well-being. Some patients may ultimately prefer amputation, given the potential complications and prolonged treatment associated with limb salvage. Surgeons must engage in open and honest discussions with patients to help them make informed decisions.
Limb salvage might be an exciting challenge for us as surgeons, but we are not the ones who will have to endure the process and live with the mental and physical toll it can take.
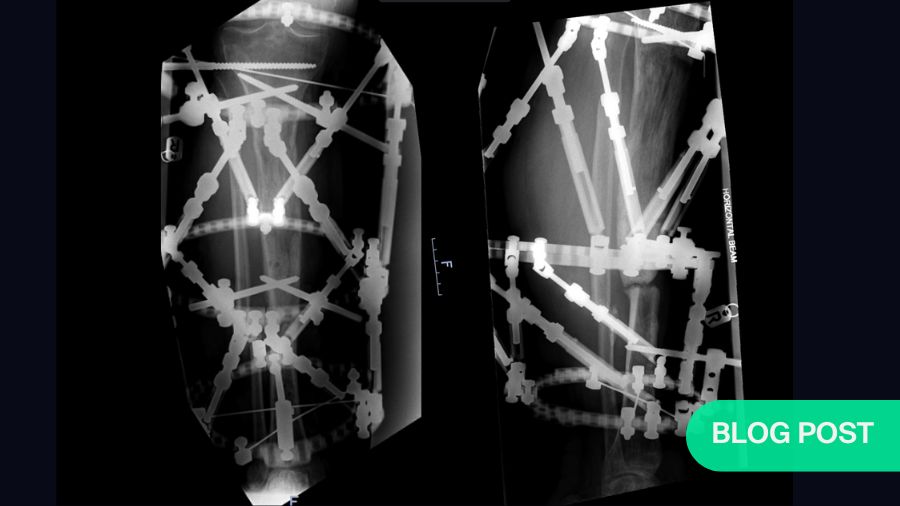
For a long time, with nasty segmental bone loss, the go-to solution was the Ilizarov method of putting on a ring fixator and doing distraction osteogenesis—literally dragging a segment of bone down to fill the bone loss gap. But, this approach has serious downsides for the patient. In an adult you can distract bone at a rate of about .75mm per day—so for a patient with bone gap of 7cm, it would take 90–100 days to do the transport, and then the patient still needs to wait for the docking site to heal and the regenerated bone to mature. This can take a further 200 days. Sometimes the bone doesn’t heal and in the worst cases s patient might endure the pain of a cage on their leg for a year, only to be told, “Sorry, but your docking site hasn’t healed.” The whole process could take more than a year, during which the patient might also experience pin site infection and additional procedures to change a pin or modify the cage., Sometimes, surgeons cynically may refer to ring fixation as a pre-amputation procedure - that isn’t entirely unfair. At the end of all this, success is still a relative term, because it looks very different to the patient than it does to the surgeon.
With a focus on the bone defect, frame surgeons can forget that to transport a segment of bone, you literally drag it through soft tissues, causing skin damage and discomfort as well as stiffness at neighboring joints. One can only imagine the discomfort. In the end, the patient is often left with dramatic longitudinal scars where the pins have dragged through the skin.
As surgeons we might get excited with the result—after all, the patient now has a straight leg, out to length, all healed up. However, from the patient’s point of view, all they see is a scarred, swollen leg prone to chronic stiffness, chronic swelling, and residual pain. They rarely love it as much as we do.


Using lengthening nails in open fractures
The lengthening nail is a new development that could prove to be a game changer and is worth mentioning in this context. It employs the same biomechanics and bone physiology as the Ilizarov method, but with purely internal fixation.
With plate assisted bone segment transport (PABST), a plate holds the limb out to length, which is also what a stacked ring fixator does. In the ring fixator, a middle segment moves to drag the piece of bone down to fill the gap, but here, it’s the lengthening nail that does the moving of the bone. It moves the middle segment from the top to the bottom at the right pace, so that distraction osteogenesis causes new bone to form in the gap. It works in the same way as a frame, but crucially it is not an apparatus on the outside of the leg with the pins dragging through the skin.
A real advantage of this method is that it makes it much easier to deal with swelling, which can be a problem. Because all the stability is internal, patients can wear pressure garments and physiotherapists can get at their leg to help manage the swelling, making the patient journey better.
The transport nails have also reduced the treatment times required. The amount of time spent in the transport phase is reduced because nails can be potentially distracted faster— distraction osteogenesis can happen at a rate of up to 1.25mm a day with fewer breaks for things like pin site infections. You therefore reach the last stage of treatment, managing the docking site, sooner. The patient is still waiting for the fracture to heal and having physiotherapy, but they are not lying in hospital or having to visit as often, which is another improvement. With the lengthening nails, the patient's contact with the hospital and the burden of being a patient is considerably reduced.
While this is a very welcome development, the functional result after all the pain and surgery is hardly ever a normal leg—and yet amazingly, so many of the studies that have investigated this area find that there is better patient satisfaction with a “foot on a stick” than with losing the leg. Many people struggle with the idea that a part of them is going to be discarded. Amputation continues to be a huge mental barrier to overcome, even if you do counsel the patients that a good prosthetic limb will give them much better function.
Amputation as an option in conversation
Amputation should not be an elephant in the room that no-one talks about, but you do have to be sensitive when you have the first conversation with the patient. The option should always be in the conversation, otherwise you might be peddling a dangerous hope to the patient. Everyone should understand that amputation is an option at every stage of the treatment, and that it’s not a sign of failure on anyone’s part. It is merely a treatment option.
It is vital to communicate this in the beginning to ensure that everyone is engaged and informed in the following treatment decision. If complications do arise during limb salvage and you must decide for amputation, there at least has been proper awareness of the possibility, and you weren’t peddling the false hope that limb reconstruction is a panacea that will always work. It also gives the patient the ability to interrupt the treatment if they are not coping with the frame or the pain, that this wasn’t what they imagined at the outset, and they’d like a change of plan.
Clear communication between the doctor and the patient is vital. Some might argue that leaving the decision to the patient is unfair as they may not fully understand all the implications, especially the risks—the risk of infection, soft tissue management, the rings, the risk of non-union, and revision nailing, non-union, a not completely functional foot with equinus contractures. Even when you discuss all implications, patients may not be sufficiently knowledgeable to dispassionately make an informed decision. Merely by giving the opportunity to go down the limb salvage route, doctors may be offering false hope.
While a patient may not have the same knowledge or experience as us, it is important to remember that we are not in their situation. There must always be a door open to revisit the conversations you had, making it clear to the patient, that even though they have decided to go for limb salvage, they are not wedded to it. And it also important to discuss alternative procedures other than the Ilizarov-type and amputation, such as various bone-graft strategies. The treatment plan can always be changed to try something else.
Another thing to remember in getting the communication and decision-making right is to involve other people, not just you and the patient. When it’s a question between amputation and salvage, make sure that you include consultation with the prosthetic service so that the patient can see what the prosthetics will look like. If possible, get them to talk to someone who can describe to them life as an amputee and give them access to other patients who have first-hand lived experiences. Hearing another patient's perspective is a wonderful support.
The importance of cross-functional care
It is also important to create a collaborative environment and include as many professionals involved as possible to provide their input in challenging clinical situations. Some practices already have formalized processes where plastic surgery, vascular surgery, orthopedic surgery, and general trauma surgery will give input, as well as infectious disease when infection is a concern. These will always be emotional journeys for the patients, so psychiatry may also need to have a say, as well as physical medicine, rehabilitation, and behavioral health.
Importantly, the patient's family must be involved as a resource and to support in the decision-making. There is so much involved with trying to save a limb, and oftentimes, limb salvage can be more destructive than amputation because of the disability, the pain medication, and the strain that puts on the family.
We may think that the outcome is going to be determined by the quality of our surgery and how advanced our surgical solution will be. But, other factors may be even more important when it comes to achieving a good outcome for the patient. Your abilities as a coach are just as important as your abilities as a surgeon.
If the patient is well-supported through the decision-making and the treatment processes, they are far more likely to have a positive attitude to what they've been through and where they arrive. And a positive attitude is key for them making the most of a terrible injury.
Watch the video:
Limb salvage or amputation in severe open fractures with bone loss—Iain McFayden and Samir Mehta discuss the patient journey (AO TV, December 2023).
About the authors:

Samir Mehta is an orthopedic trauma surgeon at the University of Pennsylvania in Philadelphia, USA. He has been recognized by Best Doctors in America in 2009–2012 and 2015–2018, along with several additional teaching awards. In addition, Dr. Mehta holds several local, national, and international leadership positions with respect to orthopedic trauma.

Iain McFadyen is an experienced consultant in Trauma and Orthopedics with a full-time trauma practice. He has a special interest in complex upper and lower limb fractures, non-union, bone infection and deformity correction. Iain was previously Chief of Trauma in Brighton, UK, where he helped lead the establishment of major trauma systems on the Southeast Coast. He is the National Director of Clinical Audit for the UK's Trauma Audit and Research Network (TARN) and co-chairman of the Fracture Guidelines Development Group for the National Institute for Health and Care Excellence (NICE).
You might also be interested in:

Competency-based AO Trauma Curriculum Courses
The AO Trauma courses ensure that the learning is focused on addressing patient problems and improving patient care.

The AO Surgery Reference
The AO’s all-in-one online reference supports you from patient assessment to aftercare in the management of a variety of fractures.
AO Trauma Guest Blog: Necrotizing fasciitis
Severe soft tissue infections are potentially life-threatening conditions. Iain McFadyen calls for a new approach.