
Fracture-related infection: Consensus recommendations on diagnosis and treatment (an AO webinar)
BY WILLEM-JAN METSEMAKERS AND MICHAEL VERHOFSTAD
Learning Objectives of the Associated Webinar
Regarding fracture-related infections (FRIs), the linked webinar will help participants:
1. To appreciate the importance of
a. a well-established diagnosis
b. the implementation of a multidisciplinary team approach.
2. To recognize/understand/appreciate
a. the main treatment principles for FRIs;
b. factors that influence surgical decision-making; and
c. how to apply up-to-date treatment strategies for FRIs. The included video demonstrations show techniques of
i. Intramedullary canal reaming
ii. Shaping and placement of an antibiotic nail in the intramedullary canal
d. the importance of patient follow-up (as demonstrated in a later phase)
Fracture-related infections (FRIs) develop in more than one-quarter of open fractures.1 In 3% of cases, they lead to amputations. However, in both translational and clinical studies, research on such musculoskeletal trauma-related infections lags behind research in orthopedic arthroplasty. This means that, while surgeons have become very good at setting fractures, many suffer from knowledge gaps on how to diagnose and treat FRIs.
To help find ways to bridge those gaps, in collaboration with the European Bone and Joint Infection Society (EBJIS), the Pro-Implant Foundation, and the Orthopedic Trauma Association (OTA), the AO Foundation hosted the FRI Consensus Group’s first meeting at the AO headquarters in Davos, Switzerland . For their first meeting, in December 2016, the participants’ long-term goal was to make more information on FRIs available to orthopedic trauma surgeons around the world through publications, websites, and apps.
The Group’s initial aim was to develop diagnostic criteria and a definition for FRI. They fulfilled this aim exceptionally well, agreeing unanimously on a set of key criteria. For example, FRI would be defined as a single phenomenon, not subdivided into acute and chronic; nor would different classifications be applied based on location or depth.
This definition differs from the CDC surgical site infection. For example, whereas the CDC sets cut-off periods for the occurrence of SSIs, the follow-up time for FRIs is indefinite. This is because an FRI can take months or even years to become noticeable.
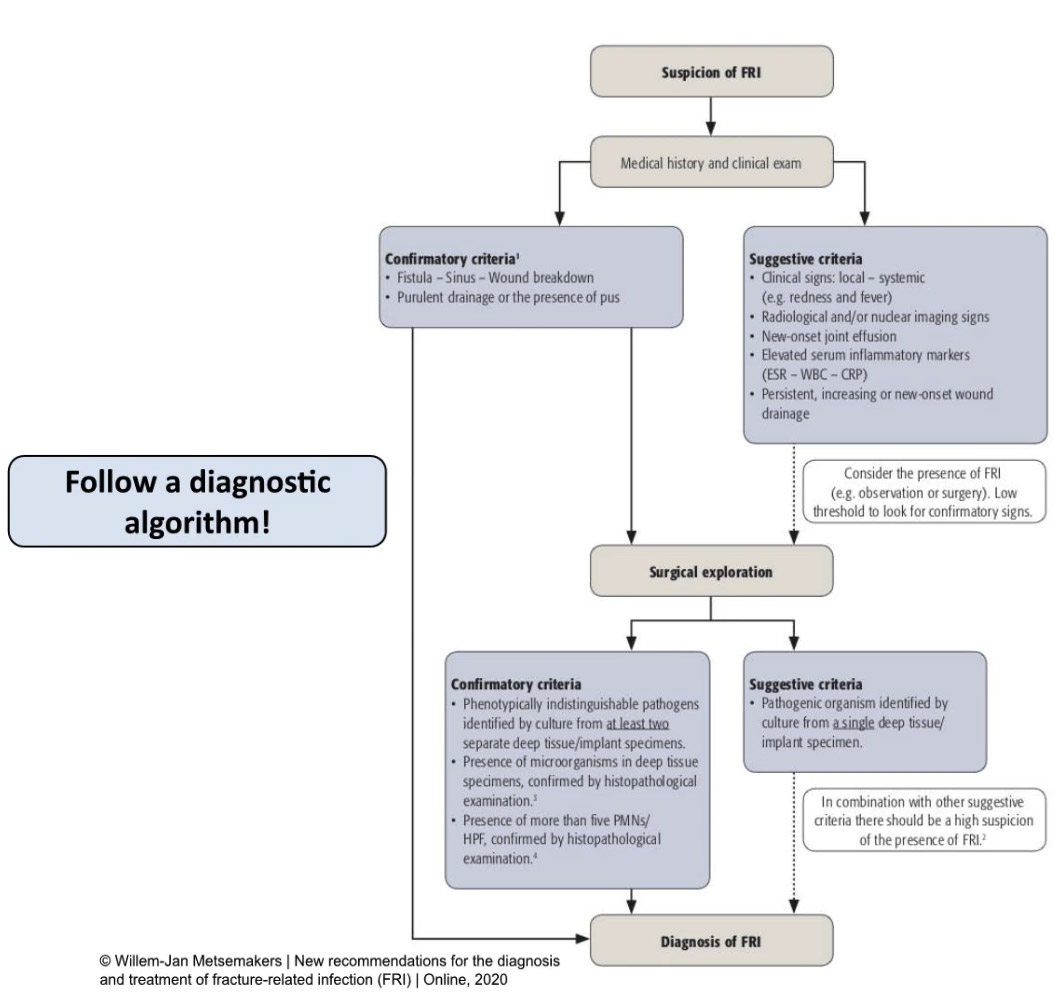
The FRI consensus definition is divided based on two levels of certainty. The first level are the confirmatory criteria. The presence of confirmatory criteria indicates that an FRI is definitely present. The second level are the suggestive criteria. The presence of these indicates a need for further testing to search for confirmatory signs.
Only two of the five confirmatory signs are visible via a clinical exam:
1. Fistula, sinus or other indications of wound breakdown. This would include any direct contact between the outside world and the bone or the implant.
2. Purulent drainage or visible pus.
Note: Surface swabs are not reliable indicators of FRIs.
The remaining three confirmatory signs require surgical exploration:
3. Phenotypically indistinguishable pathogens identified by cultures from a minimum of two separate deep tissue or implant specimens.
4. The presence of microorganisms in deep tissue (taken during operative intervention and confirmed by histopathological examination)
5. The presence of more than 5 PMN/HPF (indicated via histopathological examination)
Suggestive signs include:
1. General clinical signs such as redness, fever (systemic signs)
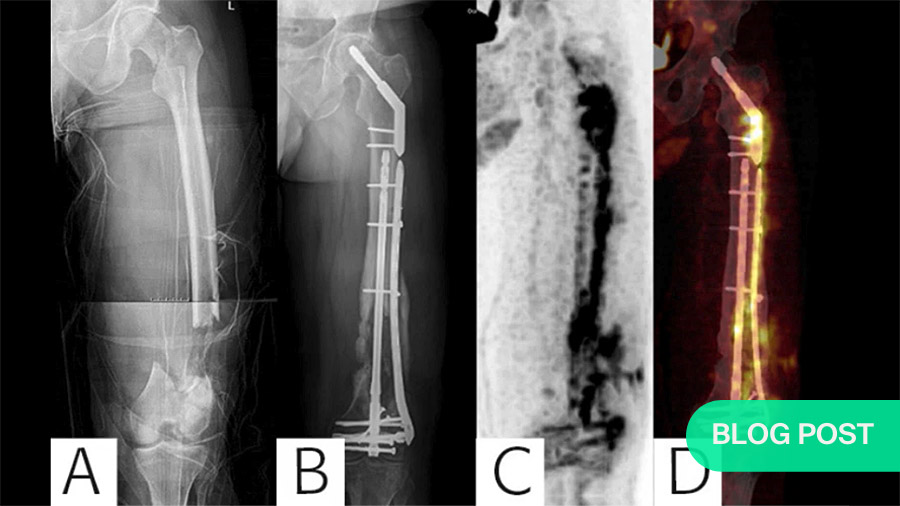
2. Radiological and/or nuclear imaging such as WBC scintigraphy showing, e.g., bone lysis around the fracture site or implant
3. New-onset joint effusion
4. Elevated serum inflammatory markers
5. Persistent, increasing or new-onset wound drainage
And with surgical exploration
6. Pathogenic organisms identified by culture from a single deep tissue/implant specimen.
Based on their work to this point, the Group produced the diagnostic algorithm shown in Figure 1 (below).
The FRI consensus is currently endorsed by many international organizations.
The FRI consensus group also worked together to isolate core principles of FRI treatment and produced an article on general treatment principles.
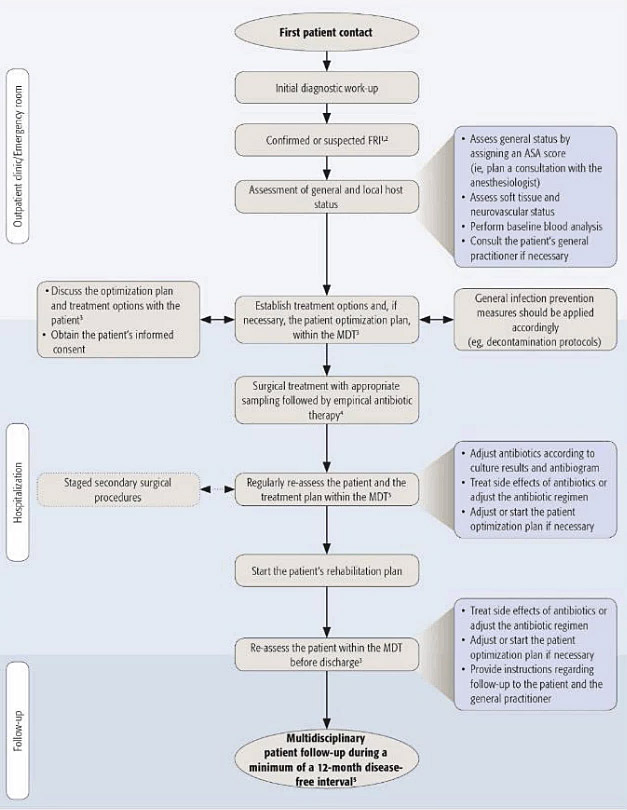
Figure 2 (below) systematizes the full set of recommended treatment steps from first patient contact to multidisciplinary patient follow-up, which takes place after a minimum 12-month disease-free interval. Regarding the composition of the multidisciplinary team (MDT), it is essential that it involve at least three disciplines: surgeons, an infectious disease specialist and an internist. Preferably, a clinical pharmacist can also be enlisted, as well as any other professions that apply to the case at hand.
For a demonstration of the Treatment Algorithm’s application, please go to the full webinar. The webinar also includes a short video of the first stage of an operation. This demonstrates a technique for quickly reaming the medullary canal with an electric reaming device. One added benefit of this process is that bone debris and other tissue extracted via reaming are usable for intramedullary tissue cultures.
As treating an FRI depends on knowing as well as possible which bacterium we’re fighting, starting off with reliable microbiological cultures is crucial. The protocols formerly validated for prosthetic joint infection and other implant-related infections can also be applied to FRIs.
Techniques for operative debridement and tissue sampling
For example, for at least two weeks before a planned surgery, all antibiotics should be avoided. During an operative debridement, at least five deep tissue samples should be taken. Each of these should be collected with unused, sterile instruments. And superficial skin or sinus tract samples should be avoided, as they have no predictive value. In fact, in spite of the temptation to explore a wound in an outpatient clinic examination room, a suspected FRI should never be swabbed locally in non-sterile conditions.
Furthermore, for samples taken under sterile conditions, histopathology has excellent confirmatory value. Morgenstern et al. (2018)1 showed, particularly in chronic late-onset cases, another strong histopathological confirmatory sign is the presence of more than five polymorphonuclear cells per high-power field.
F-FDG-PET scans or white blood cell (WBC) scintigraphy?
In addition, as non-union is suggestive of an FRI, radiological images should be examined very closely. If available, F-FDG-PET scans show high diagnostic accuracy for FRIs 2, but are only recommended 1-6 months after the initial reduction. For earlier testing, white blood cell scintigraphy 3 shows excellent diagnostic value. However, whereas F-FDG-PET imaging only requires a single scanning session, WBC scintigraphy requires two.
Whatever the results for the scans or microbiological cultures, though, none of these are 100% accurate. Therefore, trust your own eyes. Even if other tests are negative, if you see a fistula or a sinus, that’s a confirmatory sign.
Assuming that an FRI is present, considering that antibiotics will be discontinued for the two weeks leading up to the revision, the patient’s general health should be optimized well in advance. To monitor key health indicators, e.g., blood levels, kidney and liver function, as well as to stratify associated risks, the American Society of Anesthetists (ASA) physical classification is very useful. ASA scores will also help determine personalized treatment options for each patient.
This preparatory stage is also where the value of a MDT becomes clear. Particularly in cases of complex revisions, optimal outcomes are virtually impossible without input from at least three professions. In fact, in light of such teams’ importance, we recommend that complex cases be referred to specialized centers that regularly use MDTs.
The actual surgery will require soft tissue sampling, debridement, and fracture stabilization. The details of evidence-based local treatment are the topic of another paper published in JOT by the Consensus Group 4.
In case you are treating an intramedullary FRI, a second video demonstrates how to make and place an antibiotic spacer. While many techniques are available for this, all are quite cumbersome. Therefore, one of the group’s current aims is to work out a more convenient system, possibly involving a pre-fabricated antibiotic nail.
As noted above, the webinar also includes two case studies, both of which result in major long-term functional gains for the involved patients. There are also more detailed descriptions of the diagnostic-, treatment, and follow-up-related points. It concludes with a question-and-answer session. Where applicable, the answers are incorporated in this summary.
Watch a video recording of the original AO webinar:
About the authors:

Willem-Jan Metsemakers is trauma surgeon and chairman of the Department of Trauma Surgery from the University Hospital in Leuven, Belgium.

Michael Verhofstad is trauma surgeon and chairman of the Department of Trauma Surgery of the Erasmus University Medical Center in Rotterdam, the Netherlands.
Both are member of the AOTC Anti-Infection Global Expert Committee and involved in various AO infection-related projects.
AO sincerely thanks Metsemakers and Verhofstad for so generously sharing their time and knowledge.
References
- Birt M.C., Anderson D.W., Toby E.B., Wang J. Osteomyelitis: Recent advances in pathophysiology and therapeutic strategies. J. Orthop. 2016;14:45–52. doi: 10.1016/j.jor.2016.10.004. [PMC free article] [PubMed] [CrossRef] [Google Scholar] [Ref list]. From Lu, Zhang, et al., Fracture Related Infections and Their Risk Factors for Treatment Failure—A Major Trauma Centre Perspective, Diagnostics (Basel). 2022 May; 12(5): 1289. Published online 2022 May 22. doi: 10.3390/diagnostics12051289
- Bezstarosti H., Van Lieshout E.M.M., Voskamp L.W., Kortram K., Obremskey W., McNally M.A., Metsemakers W.J., Verhofstad M.H.J. Insights into treatment and outcome of fracture-related infection: A systematic literature review. Arch. Orthop. Trauma Surg. 2019;139:61. doi: 10.1007/s00402-018-3048-0. [PMC free article] [PubMed] [CrossRef] [Google Scholar] [Ref list]. From Lu, Zhang, et al., Fracture Related Infections and Their Risk Factors for Treatment Failure—A Major Trauma Centre Perspective, Diagnostics (Basel). 2022 May; 12(5): 1289. Published online 2022 May 22. doi: 10.3390/diagnostics12051289
- Mario Morgenstern et al., July 2018, The value of quantitative histology in the diagnosis of fracture-related infection. Bone and Joint Journal 100-B(7):966-972. DOI:10.1302/0301-620X.100B7.BJJ-2018-0052.R1
- Justin VC Lemans, et al., The diagnostic accuracy of 18F-FDG PET/CT in diagnosing fracture-related infections. Eur J Nucl Med Mol Imaging. 2019; 46(4): 999–1008. Published online 2018 Dec 7. doi: 10.1007/s00259-018-4218-6. PMCID: PMC6450834. PMID: 30523391
- GAM Govaert et al., High diagnostic accuracy of white blood cell scintigraphy for fracture related infections: Results of a large retrospective single-center study. Injury. Volume 49, Issue 6, June 2018, Pages 1085-1090
- Melissa Depypere et al., Recommendations for Systemic Antimicrobial Therapy in Fracture-Related Infection: A Consensus From an International Expert Group, J Orthop Trauma. 2020 Jan;34(1):30-41. doi: 10.1097/BOT.0000000000001626
The figure at top of page was published in the following paper:
Diagnosing Fracture-Related Infection: Current Concepts and Recommendations.
Govaert GAM, Kuehl R, Atkins BL, Trampuz A, Morgenstern M, Obremskey WT, Verhofstad MHJ, McNally MA, Metsemakers WJ; Fracture-Related Infection (FRI) Consensus Group. J Orthop Trauma. 2020 Jan;34(1):8-17. doi: 10.1097/BOT.0000000000001614.
Further readings
-
Read more ...
- Musculoskeletal Infection in Orthopaedic Trauma: Assessment of the 2018 International Consensus Meeting on Musculoskeletal Infection.
Obremskey WT, Metsemakers WJ, Schlatterer DR, Tetsworth K, Egol K, Kates S, McNally M; ICM Orthopaedic Trauma Work Group*; ICM Orthopaedic Trauma Work Group*.
J Bone Joint Surg Am. 2020 May 20;102(10):e44. doi: 10.2106/JBJS.19.01070.
PMID: 32118653 - Intramedullary tissue cultures from the Reamer-Irrigator-Aspirator system for diagnosing fracture-related infection.
Onsea J, Pallay J, Depypere M, Moriarty TF, Van Lieshout EMM, Obremskey WT, Sermon A, Hoekstra H, Verhofstad MHJ, Nijs S, Metsemakers WJ.
J Orthop Res. 2021 Feb;39(2):281-290. doi: 10.1002/jor.24816. Epub 2020 Aug 10.
PMID: 32735351 - Evidence-Based Recommendations for Local Antimicrobial Strategies and Dead Space Management in Fracture-Related Infection.
Metsemakers WJ, Fragomen AT, Moriarty TF, Morgenstern M, Egol KA, Zalavras C, Obremskey WT, Raschke M, McNally MA; Fracture-Related Infection (FRI) consensus group.
J Orthop Trauma. 2020 Jan;34(1):18-29. doi: 10.1097/BOT.0000000000001615.
PMID: 31464858 Free PMC article.Review. - Validation of the diagnostic criteria of the consensus definition of fracture-related infection.
Onsea J, Van Lieshout EMM, Zalavras C, Sliepen J, Depypere M, Noppe N, Ferguson J, Verhofstad MHJ, Govaert GAM, IJpma FFA, McNally MA, Metsemakers WJ.
Injury. 2022 Jun;53(6):1867-1879. doi: 10.1016/j.injury.2022.03.024. Epub 2022 Mar 12.
PMID: 35331479 - Recommendations for Systemic Antimicrobial Therapy in Fracture-Related Infection: A Consensus From an International Expert Group.
Depypere M, Kuehl R, Metsemakers WJ, Senneville E, McNally MA, Obremskey WT, Zimmerli W, Atkins BL, Trampuz A; Fracture-Related Infection (FRI) Consensus Group.
J Orthop Trauma. 2020 Jan;34(1):30-41. doi: 10.1097/BOT.0000000000001626.
PMID: 31567902 Free PMC article. - Diagnostic challenges and future perspectives in fracture-related infection.
Morgenstern M, Kühl R, Eckardt H, Acklin Y, Stanic B, Garcia M, Baumhoer D, Metsemakers WJ.
Injury. 2018 Jun;49 Suppl 1:S83-S90. doi: 10.1016/S0020-1383(18)30310-3.
PMID: 29929701 Review. - The Incidence of Fracture-Related Infection in Open Tibia Fracture with Different Time Interval of Initial Debridement.
Hadizie D, Kor YS, Ghani SA, Mohamed-Saat MA.
Malays Orthop J. 2022 Nov;16(3):24-29. doi: 10.5704/MOJ.2211.005.
PMID: 36589367 Free PMC article. - General treatment principles for fracture-related infection: recommendations from an international expert group.
Metsemakers WJ, Morgenstern M, Senneville E, Borens O, Govaert GAM, Onsea J, Depypere M, Richards RG, Trampuz A, Verhofstad MHJ, Kates SL, Raschke M, McNally MA, Obremskey WT; Fracture-Related Infection (FRI) group.
Arch Orthop Trauma Surg. 2020 Aug;140(8):1013-1027. doi: 10.1007/s00402-019-03287-4. Epub 2019 Oct 29.
PMID: 31659475 Free PMC article. - Diagnosing Fracture-Related Infection: Current Concepts and Recommendations.
Govaert GAM, Kuehl R, Atkins BL, Trampuz A, Morgenstern M, Obremskey WT, Verhofstad MHJ, McNally MA, Metsemakers WJ; Fracture-Related Infection (FRI) Consensus Group.
J Orthop Trauma. 2020 Jan;34(1):8-17. doi: 10.1097/BOT.0000000000001614.
PMID: 31855973 Free PMC article. - Fracture-related infection: A consensus on definition from an international expert group.
Metsemakers WJ, Morgenstern M, McNally MA, Moriarty TF, McFadyen I, Scarborough M, Athanasou NA, Ochsner PE, Kuehl R, Raschke M, Borens O, Xie Z, Velkes S, Hungerer S, Kates SL, Zalavras C, Giannoudis PV, Richards RG, Verhofstad MHJ.
Injury. 2018 Mar;49(3):505-510. doi: 10.1016/j.injury.2017.08.040. Epub 2017 Aug 24.
PMID: 28867644 - Fracture-related infection.
Moriarty TF, Metsemakers WJ, Morgenstern M, Hofstee MI, Vallejo Diaz A, Cassat JE, Wildemann B, Depypere M, Schwarz EM, Richards RG.
Nat Rev Dis Primers. 2022 Oct 20;8(1):67. doi: 10.1038/s41572-022-00396-0.
PMID: 36266296 Review. - Pathogenesis and management of fracture-related infection.
Depypere M, Morgenstern M, Kuehl R, Senneville E, Moriarty TF, Obremskey WT, Zimmerli W, Trampuz A, Lagrou K, Metsemakers WJ.
Clin Microbiol Infect. 2020 May;26(5):572-578. doi: 10.1016/j.cmi.2019.08.006. Epub 2019 Aug 22.
PMID: 31446152 Review. - Infection after fracture fixation: Current surgical and microbiological concepts.
Metsemakers WJ, Kuehl R, Moriarty TF, Richards RG, Verhofstad MHJ, Borens O, Kates S, Morgenstern M.
Injury. 2018 Mar;49(3):511-522. doi: 10.1016/j.injury.2016.09.019. Epub 2016 Sep 11.
PMID: 27639601 Review. - Fracture-related infection.
Baertl S, Metsemakers WJ, Morgenstern M, Alt V, Richards RG, Moriarty TF, Young K.
Bone Joint Res. 2021 Jun;10(6):351-353. doi: 10.1302/2046-3758.106.BJR-2021-0167.R1.
PMID: 34076501 Free PMC article.No abstract available. - Definition and diagnosis of fracture-related infection.
McNally M, Govaert G, Dudareva M, Morgenstern M, Metsemakers WJ.
EFORT Open Rev. 2020 Oct 26;5(10):614-619. doi: 10.1302/2058-5241.5.190072. eCollection 2020 Oct.
PMID: 33204503 Free PMC article.Review. - Bone infection: a clinical priority for clinicians, scientists and educators.
Moriarty TF, Muthukrishnan G, Daiss JL, Xie C, Nishitani K, Morita Y, Awad H, de Mesy Bentley KL, Masters E, Bui T, Yan M, Owen J, Mooney B, Gill S, Puetzler J, Wenke JC, Morgenstern M, Metsemakers WJ, Noll C, Joeris A, Richards RG, Schwarz EM, Kates SL.
Eur Cell Mater. 2021 Oct 18;42:312-333. doi: 10.22203/eCM.v042a21.
PMID: 34661245 Review.
- Musculoskeletal Infection in Orthopaedic Trauma: Assessment of the 2018 International Consensus Meeting on Musculoskeletal Infection.
You might also be interested in:

AO Surgery Reference
AO Surgery Reference is your go-to resource for the management of fractures, based on current clinical principles, practices, and available evidence.

myAO
Join AO's digital network! On myAO, you can securely save and share cases, connect and exchange knowledge with peers, and access leading clinical and scientific expertise.

AO video hub
Discover a wealth of educational videos, practical exercises, recorded webinars, expert presentations, and interviews from AO's world-renowned faculty.