
What I wish I had known earlier about metacarpal fractures: the never-ending fight between malunion and stiffness
BY DR VOJTĚCH KUNC

Why do some “simple” metacarpal fractures produce unhappy patients, while some ugly-looking fractures do surprisingly well? The answer is usually not in the radiograph; it’s in function, malunion (rotation, shortening, angulation) and stiffness.
I used to treat metacarpals like small long bones. Over time, metacarpals taught me a different lesson: treat the hand, not the metacarpal. The hand forgives some deformity, but especially around the metacarpophalangeal (MCP) joints, it does not forgive rotation or stiffness. The “rules” about acceptable malunion matter far less than we think, unless we understand why they exist and when they stop applying.
-
Read the quick summary:
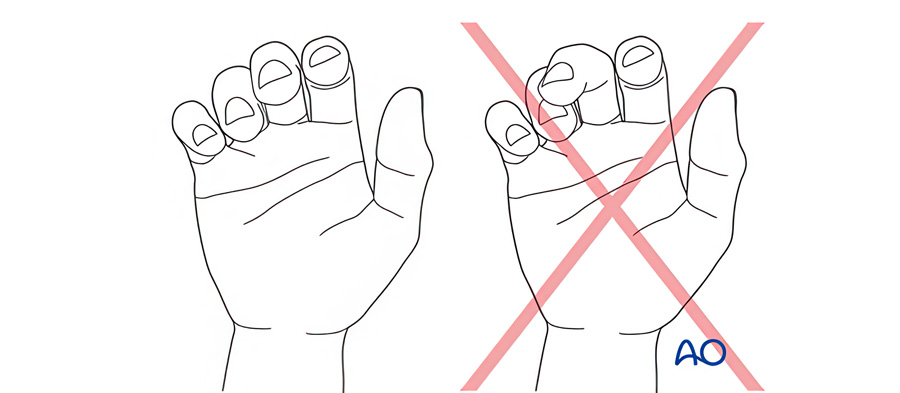
- Rotation is always a problem. Check it clinically – best seen on finger flexion (cascade/scissoring), but least affected by edema in extension.
- Shortening and angulation lead to loss of grip strength, but the clinical impact depends on the patient's demands and the involved ray.
- Splinting is a treatment; over-splinting is a complication. Many bad outcomes are iatrogenic stiffness.
- Internal fixation should allow motion. Choose the least invasive method that gives stability for early protected movement.
- Every plan chooses a side in the fight: risking malunion vs risking stiffness. The best plan is patient specific.
Disclaimer: The article represents the opinion of individual authors exclusively and not necessarily the opinion of AO or its clinical specialties.
The central problem: malunion vs. stiffness
Hand fracture care is one big battle between two life-long enemies: malunion and stiffness. We often choose the lesser evil. We try to hide behind textbook thresholds, “acceptable angulation”, “acceptable shortening”, but the fight is often lost due to the lack of understanding what lies behind those rules.
Only once we understand the mechanism, the real question can be answered: Which risk is more harmful for this patient, residual deformity or loss of motion? Then we can tailor treatment to the patient’s demands.
1. Rotation rules everything
The most reliable examination is in flexion, because that is when rotation becomes functionally obvious. This is the non-negotiable examination. Simply said: “All is ruled by the rotation.”
We are often hesitant to remove the cast at 5–7 days after reduction, fearing we will lose alignment. But if we never reassess rotation, we risk missing the one deformity the hand tolerates least.
Edema can change posture and make the little finger look deceptively internally rotated. If we are unable to reduce the edema in a week, it is good to know that edema has less effect on the nail plate orientation in extension as shown by Smith and colleagues.
2. Shortening: when does it matter clinically?
Unacceptable shortening is often framed as a single number—2, 3, or 5 mm depending on the textbook—presented almost like a law. In reality, it behaves like most things in hand surgery, it depends.
Biomechanical work has suggested measurable consequences. Strauch and colleagues reported increasing extensor lag with shortening, and Mejia and colleagues reported a reduction in grip strength with shortening. Clinically, I find the grip-strength question more relevant than extensor lag for many patients because most hands have some MCP hyperextension reserve.
3. Angulation: the never-ending debate
The debate about acceptable angulation of metacarpals is likely never-ending, especially for the 5th metacarpal, where acceptable values in the literature and in practice vary widely (between 20° to 70°+). It was shown by Ali and colleagues that 30° of angulation led to 92% of grip strength in the little finger. Is this a reason to operate? Again, it depends.
It is rare, but to some patients, the aesthetics of “loss knuckle” due to angulation matters. In some nations, the hands are checked during enlistment to the army, and the appearance of a “lost knuckle” might be problematic.
Shortening and angulation in different rays:
Shortening and angulation affect each finger differently, making it essential to tailor assessment and management to the specific ray involved.
- Shortening and angulation tend to matter more in the ulnar rays (4th and 5th) for grip strength, especially in high-demand hands.
- The central rays (2nd and 3rd) have different stability constraints at the carpometacarpal (CMC) joints and behave differently in deformity tolerance.
4. When should I fix and why?
If we understand this, we can tailor the treatment to our patient. For example, patients with low functional demands and low treatment adherence, often those injured in street brawls, will tolerate quite well both the angulation and shortening, as the quality of the fist-punch does not matter. On the other hand, the same injury in a professional boxer will lead to significantly decreased quality of the punch (lower fist strength, altered punch landing surface, etc.)
5. Read more about the treatment: AO Surgery Reference
For readers who want a structured overview of treatment options and aftercare principles, AO Surgery Reference has dedicated guidance for adult metacarpal fractures.
6. Stiffness is the worst loss
Nothing ruins outcomes more reliably than stiffness. When treating conservatively, we balance on the edge: take the splint off too early, and risk losing alignment – keep it too long, and we create stiffness.
This decision is an art and difficult to explain. Everybody develops stiffness differently. I try not to leave a rigid cast for more than three weeks, but this rule is often broken in fear of secondary malalignment. Obvious help comes from buddy taping and a small orthosis to fix the palm and leave the fingers able to move.
7. The metacarpal decision pyramid: avoiding heavy metal
Prominent dorsal implants and soft-tissue irritation can drive stiffness. That doesn’t mean plates are “bad”. It means we should be honest about the trade-offs: stability, soft tissue, and the ability to start motion.
I find it helpful to borrow a concept from the reconstructive surgery pyramid: choose the least invasive effective option.
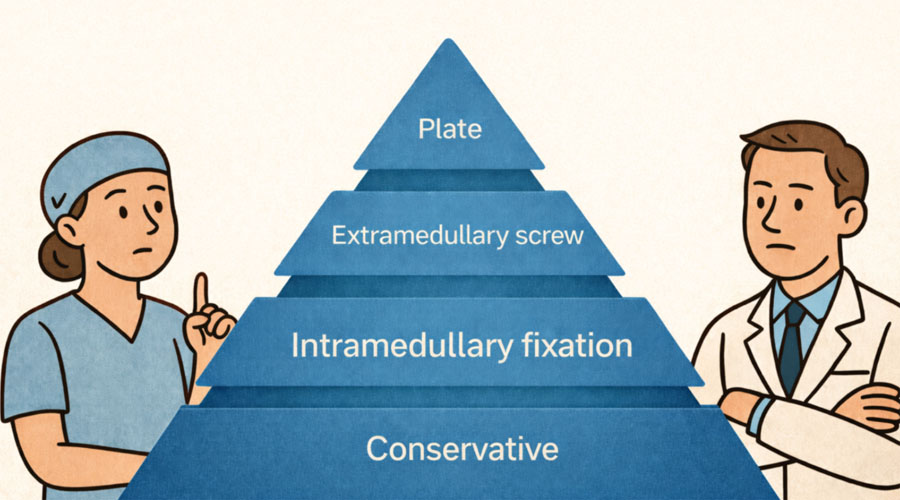
From least invasive to most invasive:
- Conservative management (best when stable and without malrotation)
- Intramedullary fixation (when suitable patterns allow it; aim: stability with minimal soft-tissue disruption)
- Extramedullary screws
- Plate fixation (valuable when comminution and other techniques cannot achieve stability and early motion, but highest risk of stiffness)
The point is to ask: Can I achieve the stability I need for early motion with less invasive method? If yes, the hand often thanks you later.
(And a fair note: in some situations, a well-chosen plate that enables early mobilization can produce excellent outcomes—especially if soft tissue is respected and rehab is planned.)
Principles for optimal fracture management
- Effective fracture management relies on a few fundamental principles that help guide clinical decisions and optimize patient outcomes.
- Rotation is never acceptable. Check it clinically, best in flexion, and re-check after swelling improves.
- Shortening and angulation matter, but context matters more. Use “numbers” as guidance, not commandments.
- Splinting is treatment. Over-splinting is a complication. Plan motion from day one.
- Fixation should serve early motion. Choose the least invasive stable option that fits the fracture and the patient.
About the author:

MUDr Vojtěch Kunc, Ph.D., is an orthopaedic trauma and hand surgeon in Prague, Czech Republic. He practices at the University Hospital Motol and serves as an academic staff member at the Institute of Anatomy, Charles University, where he leads the Hand Surgery Biomechanical Laboratory.
His clinical practice focuses on acute trauma of the upper extremity, particularly hand and wrist fractures. His research interests lie in clinically relevant anatomy and biomechanics, with 50+ publications in peer-reviewed journals and experience as a reviewer and editorial board member.
Dr Kunc has been a member of AO Trauma since 2021 and an AO Trauma Faculty member since 2024, contributing primarily to courses in hand and wrist fracture management.
Further reading:
- Smith NC, Moncrieff NJ, Hartnell N, Ashwell J. Pseudorotation of the little finger metacarpal. J Hand Surg Br. 2003; 28(5):395-398.
- Strauch RJ, Rosenwasser MP, Lunt JG. Metacarpal shaft fractures: the effect of shortening on the extensor tendon mechanism. J Hand Surg Am. 1998;23(3):519-523.
- Meija A, Lichtig AE, Ghosh A, Balasubramaniyan A, Mass D, Amirouche F. The effect of metacarpal shortening on finger strength and joint motion: A cadaveric biomechanical study. J Hand Surg Glob Online. 2023; 5(4):407-412.
- Ali A, Hamman J, Mass DP. The biomechanical effect of angulated boxer’s fractures. J Hand Surg Am. 1999; 24(4):835-844.
You might also be interested in...

AO Surgery Reference
AO Surgery Reference is a resource for the management of fractures, based on current clinical principles, practices and available evidence.

Fracture Management Essentials
The AO Trauma Online Course—Basic Principles of Fracture Management Essentials provides lectures, readings and resources, practical exercise videos, and simulations.

Fixation of Hand and Wrist Fractures
The AO Trauma Course—Introduction to Internal Fixation of Hand and Wrist Fractures concentrates on internal fixation of fractures and skeletal reconstruction procedures.

Management of hand and wrist fractures
The AO Trauma Masters Course—Management of Hand and Wrist Fractures increases knowledge and skills for managing difficult and complex hand and wrist cases.