
Trifocal femur fracture: where do I start?
BY DR GIOVANNI LONGO
Ipsilateral multifocal femoral fractures often present a challenge for the surgeon, as there is limited consensus in the literature regarding the optimal management of this rare type of fracture. In this clinical case, Dr Giovanni Longo highlights the issues he encountered while operating on this particularly challenging case. He won the Bonevoyage 2024 competition on myAO with this example case.
Disclaimer: The article represents the opinion of individual authors exclusively and not necessarily the opinion of AO or its clinical specialties.
Non-contiguous ipsilateral femoral fractures involving the proximal femur, diaphysis, and distal femur are generally associated with high-energy trauma and are poorly described in the literature. Intracapsular femoral neck fractures and complete distal intra-articular fractures (AO/OTA type 33-C) [1] present a more complex clinical picture and are even more rarely documented. Given the rarity and complexity of these injuries, there is no consensus on their optimal surgical management.
Case report, preoperative planning, and surgical management
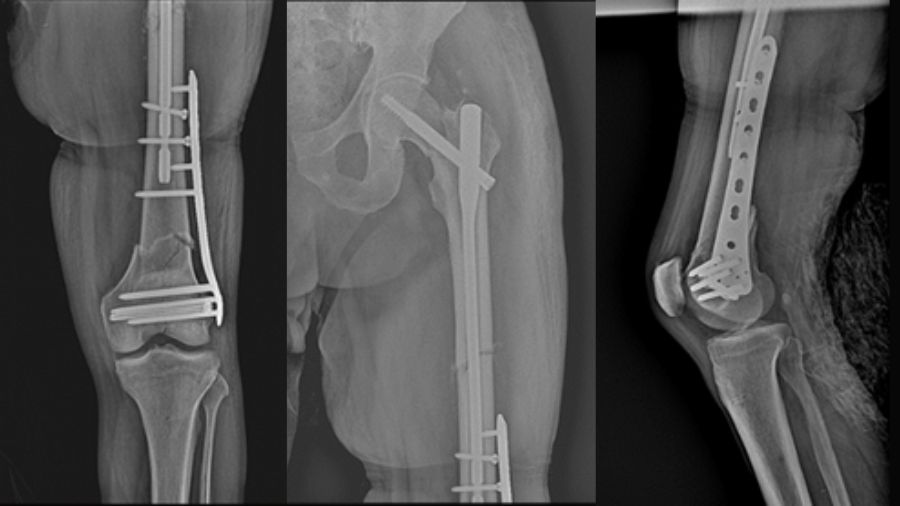
This case report describes a high-energy trifocal femoral fracture (intracapsular femoral neck, femoral shaft, and complete distal articular femur) treated with an intramedullary nail, free cannulated screws, and a LISS plate.
This combination of implants, not previously reported in the literature, allowed for an anatomical reduction with absolute stability of the distal periarticular fracture and a functional reduction with relative stability in the other two fractures (shaft and femoral neck).
The patient was a 72-year-old otherwise healthy man involved in a high-energy motor vehicle accident. On physical examination, he presented with pelvic tenderness, a shortened and externally rotated left lower limb, a swollen knee, and intact pulses.
Initial diagnostic tests revealed a left basal pneumothorax with bilateral pleural effusion, fractures of the left fifth to eighth ribs, xiphoid process fracture, nasal bone fractures, and a trifocal fracture of the left femur. He was admitted to the trauma unit at our hospital.
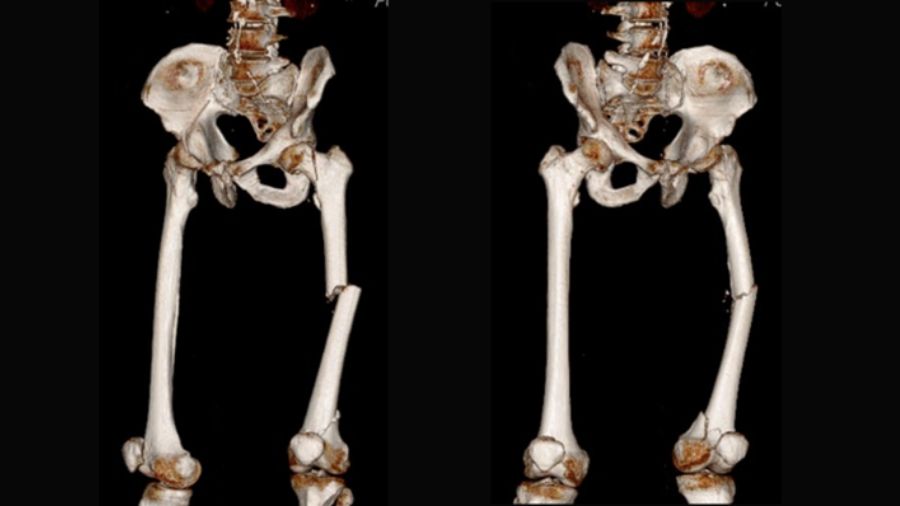
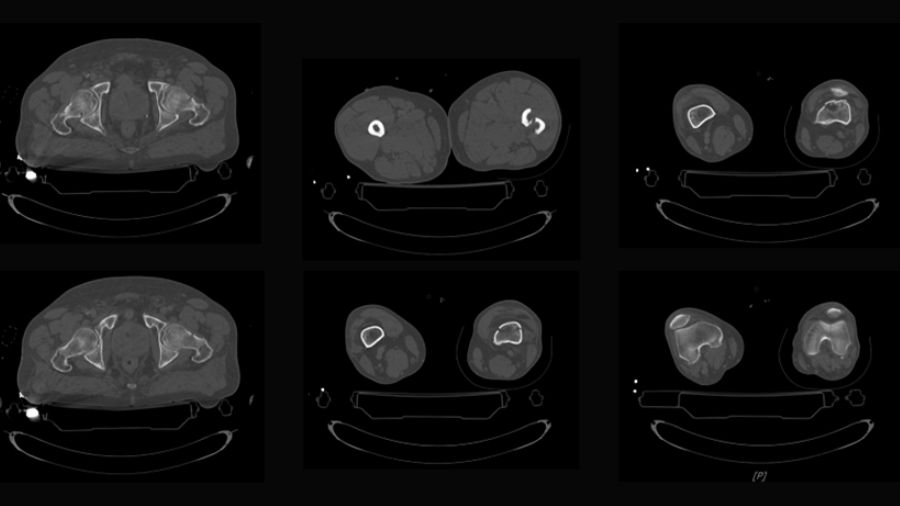
The trifocal femoral fracture (Figure 1) was classified as an obliquely oriented transcervical femoral neck fracture (AO/OTA 31-B2), a displaced shaft fracture (AO/OTA 32-A2), and a supracondylar fracture with intra-articular extension (AO/OTA 33-C2).
The left lower limb was initially treated following the principles of Damage Control Orthopedics (DCO) with tibial traction and was later admitted to the Intensive Care Unit.
The patient also had a pulmonary contusion complicated by bacterial infection and a traumatic brain injury with a right temporobasal hematoma.
After resolving the pulmonary complications, the definitive surgery was performed in a single stage, step by step:
- Kirschner wires were used to stabilize the femoral head, preventing further displacement
- Cannulated screws were applied to fix the intra-articular distal femoral fracture
- A nail with static distal locking was inserted
- A LISS plate was applied
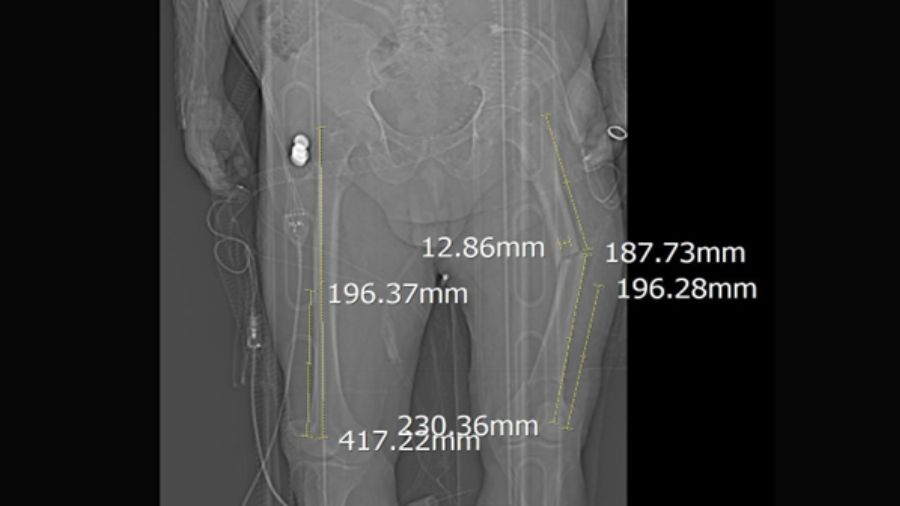
Preoperative planning
Postoperative Rehabilitation Protocol
The patient remained non-weight bearing for the first month post-surgery and immediately began physiotherapy to restore hip and knee range of motion and strengthen the quadriceps and gluteal muscles bilaterally.
Progressive weight-bearing was allowed afterward, as tolerated, until full weight-bearing was achieved.
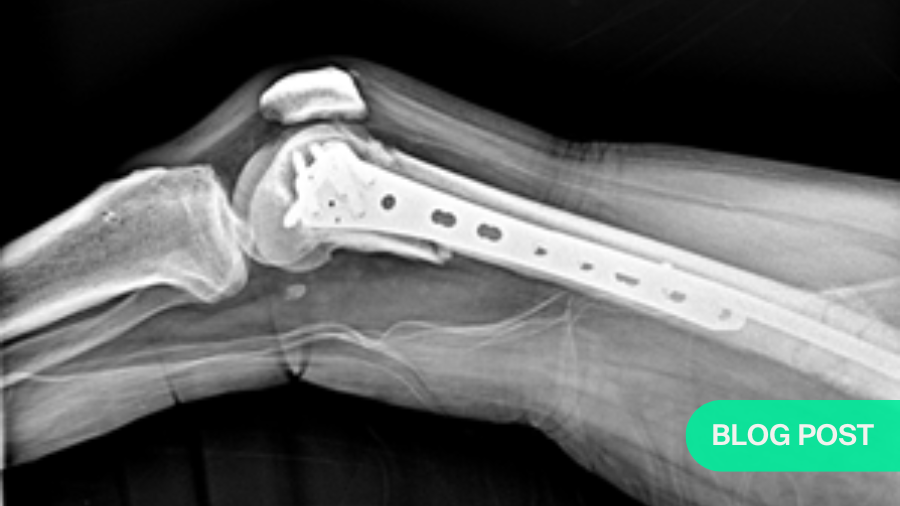
Results
As seen in the following images, all fracture sites healed with near-complete functional recovery, and no complications or deficits were reported. The full clinical case, including a video demonstrating the patient's functional recovery, can be accessed via this link.


Discussion
Trifocal femoral fractures involving the proximal, diaphyseal, and distal femur are extremely rare. Only nine cases of trifocal femoral fractures with AO/OTA type C distal fractures have been reported in the literature [2-8], with only two cases including an intracapsular femoral neck fracture [2, 3]. The case presented in this report is therefore one of the few published examples of trifocal femoral fractures comprising femoral neck, diaphyseal, and type C distal fractures [9].
Due to the rarity of this injury, there is little consensus on the surgical strategy and choice of implant. The first reported case of this injury, published by Käch in 1993, described a basicervical fracture treated with traction screws, a mid-diaphyseal fracture treated with an antegrade nail, and a type C distal femur fracture treated with a 95° blade plate, without complications [3].
In 2011, Dousa et al. reported a transcervical fracture treated with a dynamic hip screw, with mid-diaphyseal and type C distal femoral fractures treated with a 95° condylar plate, requiring reoperation for diaphyseal malunion [4].
We used an antegrade reconstruction nail for the femoral neck and diaphyseal fractures, cannulated screws for the distal intra-articular fracture, and a LISS plate for the supracondylar femur fracture. This combination prioritizes articular fractures with direct reductions and optimally treats the femoral shaft with intramedullary nailing.
However, it is important to note that the use of a single fixation device for both the femoral neck and shaft fractures may present a problem. If one of the two fractures failed to heal, it would have been necessary to revise the single fixation device, risking the healing of the other fracture sites.
Additionally, in our case, the intracapsular femoral fracture, whose fixation relied solely on the cephalic screw of the intramedullary nail, was at risk of rotational displacement.
Previous dogmas and reports have focused on prioritizing proximal and distal fractures, sometimes at the expense of the femoral shaft, under the premise that nonunion or malunion of the shaft is easier to treat than a problem in one of the terminal segments. While this may be true for the surgeon, the patient may still experience significant morbidity from this approach. With modern implants, it is possible to optimize the management of each fracture component, providing the patient with the best chance of healing without complications.
Conclusion
This case report describes a trifocal femoral fracture with intracapsular femoral neck, diaphyseal, and complete distal articular fractures surgically treated with a combination of implants not yet described in the literature. This patient achieved a favorable clinical outcome and fracture healing without complications. We believe this case may be valuable for surgeons encountering and preparing to treat similarly complex injuries.
About the author:
References and further reading:
- Meinberg EG, Agel J, Roberts CS, Karam MD, Kellam JF. Fracture and Dislocation Classification Compendium-2018. J Orthop Trauma. 2018;32 Suppl 1:S1-S170. doi:10.1097/BOT.0000000000001063
- Käch K. Kombinierte Frakturen des Schenkelhalses mit Femurschaftfrakturen [Combined fractures of the femoral neck with femoral shaft fractures]. Helv Chir Acta. 1993;59(5-6):985-992.
- Douša P, Bartoníček J, Luňáček L, Pavelka T, Kušíková E. Ipsilateral fractures of the femoral neck, shaft and distal end: long-term outcome of five cases. Int Orthop. 2011;35(7):1083-1088. doi:10.1007/s00264-010-1108-3
- Palarcík J, Nestrojil P, Bucek P. Rekonstrukcní nitrodrenový femorální hreb (Nový implantát k syntéze soucasných zlomenin tĕla a krcku téhoz femoru firmy Medin, a.s.--predbĕzná informace [Reconstruction with intramedullary femoral nailing (a new implant made by Medin, A.S. for synthesis of concurrent fractures of the femoral shaft and neck--preliminary report)]. Rozhl Chir. 1995;74(6):305-308.
- Bartoníček J., Stehlík J., Douša P. Ipsilateral fractures of the hip, femoral shaft, distal femur and patella. Hip Int. 2000;10(3):174–177.
- Griffin M, Dick AG, Umarji S. Outcomes after trifocal femoral fractures. Case Rep Surg. 2014;2014:528061. doi:10.1155/2014/528061
- Papaioannou I, Baikousis A, Korovessis P. Trifocal Femoral Fracture Treated With an Intramedullary Nail Accompanied With Compression Bolts and Lag Screws: Case Presentation and Literature Review. Cureus. 2020;12(5):e8173. Published 2020 May 17. doi:10.7759/cureus.8173
- Zhang JH, Liu H, Xu WZ, Song W, Wu J. Application of bridge-link type combined fixation system in the treatment of trifocal femoral fractures. Int Orthop. 2023;47(11):2851-2857. doi:10.1007/s00264-023-05933-4
- Robinson CA, Fitzpatrick E, Soles G, Saiz A, Lee MA, Campbell ST. Trifocal femur fracture with intracapsular femoral neck, open diaphyseal, and distal complete articular fractures. Trauma Case Rep. 2024;51:100999. Published 2024 Mar 21. doi:10.1016/j.tcr.2024.100999
You might also be interested in:

myAO
myAO gives you access to relevant, trusted sources of knowledge, moderated case discussions, and expertise across the AO’s specialties. A community trusted by over 88,000 verified surgeons worldwide.
AO/OTA Fracture and Dislocation Classification
Explore the resources and tools available that will help you classify fractures in adults and children, and find out more about the practical AO Trauma clinical tools available.

AO Trauma courses and events
AO Trauma is renowned for its professional courses targeted at orthopedic trauma surgeons and operating room personnel (ORP). Webinars and webcasts are popular additions to the event portfolio.

AO Trauma Guest Blog
Bringing together experts from the Trauma surgery community to share their perspectives, experiences, and insights. Read articles and case studies, or submit your own post proposal and promote your work to a worldwide expert community.