
Subluxation after terrible triad fixation: key insights and solutions
AO TRAUMA WEBINAR
Strategies for revising subluxated elbows after terrible triad fixation and ensuring a stable, durable initial repair are challenging. Managing such advanced injuries in older patients are especially complex. In one of the most popular AO Trauma webinars, Lars Müller from the University of Cologne Trauma Centre used five real-world case studies to discuss the strategies, to determine how to address terrible triad lesions, detecting instability early after terrible triad lesions, and prevention tips.
The recording of the webinar further outlines operative stabilization of the radial/ulnar and anterior side of the elbow if subluxed after terrible triad fixation, with videos of approaches and plating techniques.
Disclaimer: The article represents the opinion of individual authors exclusively and not necessarily the opinion of AO or its clinical specialties.
The aim of terrible triad fixation is the restoration of bony stabilizing structures (radial head and coronoid process) and lateral collateral ligament reconstruction. A surgical approach is recommended with persistent posterolateral instability following lateral collateral ligament reconstruction or when fixation of a large coronoid process fragment is indicated. The use of an external fixator is only advocated in case of persistent instability following the reconstruction of bony and ligamentous structures.
Video: AO Trauma Webinar—Subluxation After Terrible Triad Fixation. Lars Peter Müller and Michael Plecko present a live interactive webinar about subluxation after terrible triad fixation.
What is a terrible triad injury?
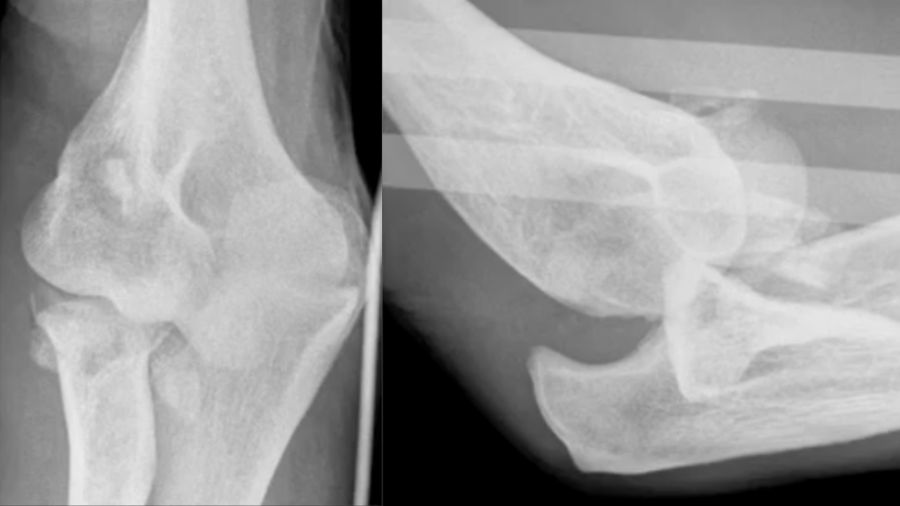
A "terrible triad" refers to a severe and complex elbow injury that involves three key elements: coronoid process fracture, radial head fracture, and elbow dislocation (either anterior or posterior). This type of injury can lead to chronic instability and complications after surgery, particularly subluxation, which is common following terrible triad fixation. Here I will demonstrate how to address post-surgery subluxation and share tips on how to identify and correct potential sources of instability during the initial surgery to avoid the need for re-operation.
Common causes of postoperative subluxation
Several factors can contribute to subluxation after a terrible triad repair. These include:
- Overstuffing of the radial head prosthesis leading to improper joint mechanics.
- Understuffing and unresolved ligament issues, often due to insufficient ligament repair.
- Anterior shifts post external fixation, when the distal humerus lacks adequate anterior support after external fixation.
- Large, unfixed coronoid fragments, leading to an unstable joint that requires further surgical intervention.
Basic principles of terrible triad fixation
For a stable elbow joint following a terrible triad injury, the key areas of focus include:
- Coronoid process
- Radial head and column
- Medial collateral ligament (MCL)
- Lateral collateral ligament (LCL)
Coronoid process
The coronoid remains one of the most challenging aspects of terrible triad injuries. There's still no consensus on which specific types of coronoid fractures must be fixed, in certain cases, fixation is essential for joint stability.
In practice, I always opt to reconstruct the radial head and column and avoid radial head resections. Additionally, when dealing with subluxation, it’s often the medial ligament that has been neglected during the initial repair. For many patients, both the lateral ligament and the extensor muscles on the lateral humerus need re-anchoring.
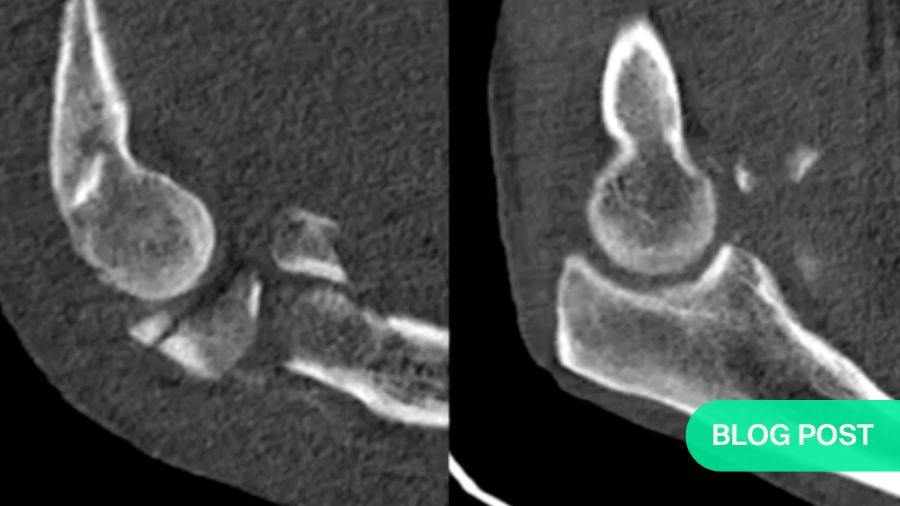
The coronoid fracture: classifying the damage
Shaun O’Driscoll’s coronoid classification system assesses the severity of coronoid fractures. The location and size of the fracture play a critical role in determining the treatment plan. For instance, a radial-sided tip fracture may not have as much impact on stability as a fracture involving the anteromedial facet.
The images demonstrate various coronoid fracture patterns, from minor tip fractures to complex fractures that involve multiple areas of the coronoid. Understanding the exact nature of these fractures—often via CT scans—is essential for effective treatment planning.
Biomechanics of the terrible triad
Conducting high-speed filming of cadaveric elbow joint simulations help better understand the biomechanical forces at play during terrible triad injuries. These slow-motion videos show how the radius and coronoid are affected by high-energy trauma, leading to fractures and ligament damage, providing a very slow-motion view of the damage unfolding.
Interestingly, coronoid tip fractures play a relatively minor role in joint stability compared to more extensive ligamentous damage, especially involving the medial collateral ligament (MCL). Research by Beingesser and Graham King suggests that MCL repair is far more important for stability than fixing the coronoid tip.
The radial head and ligaments: key considerations
The radial head, together with the coronoid, forms the anterior buttress of the elbow joint. If the radial head has an anterior rim fracture, combined with a transverse coronoid fracture, the entire anterior buttress of the elbow is compromised. This requires careful management, either through open reduction internal fixation (ORIF) or the use of a radial head prosthesis.
Regarding ligaments, subluxation following terrible triad surgery is often due to inadequate ligament repair, particularly on the medial side. In many cases, the lateral collateral ligament (LCL) is also detached, contributing to the instability.
Ligament refixation techniques
To address ligamentous instability, meticulous repair techniques are crucial. For the lateral ligament, using Krackow sutures or transosseous fixation is recommendable. These suturing techniques help secure the ligaments and prevent posterolateral instability. However, over-tightening the lateral sutures can lead to medial gapping, so careful attention is needed when tightening knots, especially during the final stages of surgery.
Postoperative therapy and protocols
Post-surgery, some extension loss is common, the importance of starting early mobilization cannot be overlooked. Overhead motion protocols—where patients are encouraged to start moving their elbow within a day of surgery—are key to achieving good flexion results. The patient must take an active role, with minimal assistance from therapists.
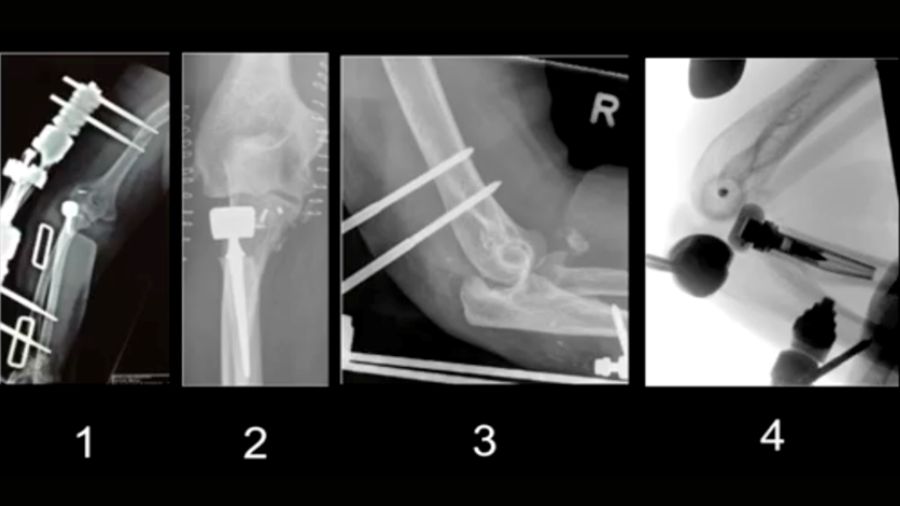
Case studies: real-world solutions in terrible triad cases
In the related recording several case studies are presented to demonstrate the principles and techniques discussed above.
Case 1: Overstuffing and medial gapping

In this case, an overstuffed radial head prosthesis led to a 1 cm elevation of the implant, causing subluxation. The video shows how to correct the prosthesis height, re-anchor the ligaments, and brace the radial head.
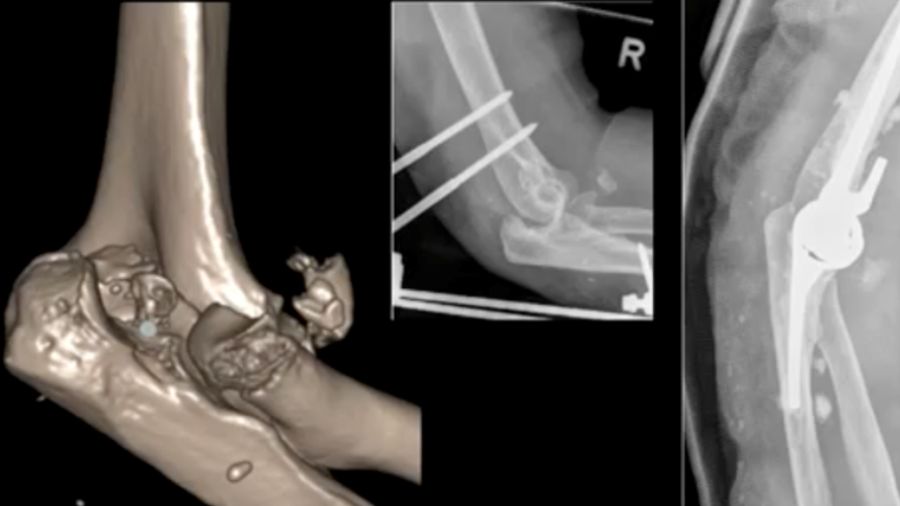
Case 2: 48-year-old male, fall from scaffold
A 48-year-old man presented with a luxated elbow, radial head fracture, and coronoid fracture. Despite initial surgery, a second CT scan revealed improper positioning of the radius head and a lateral shift in the elbow. Revised surgery was performed by fixing the coronoid plate and reattaching the lateral ligaments.
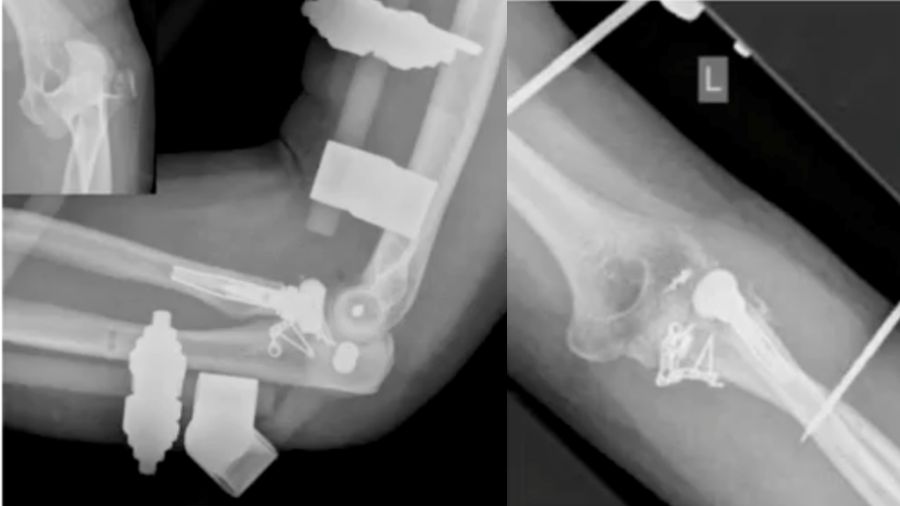
Case 3: 88-year-old woman
An 88-year-old patient with a terrible triad had an external fixator placed. A cemented prosthesis was chosen due to her age but encountered complications with cement leakage. Thankfully, no neurovascular damage occurred.
Case 4: 94-year-old woman

In this case, a total elbow prosthesis was chosen for a 94-year-old patient with severe trauma. The prosthesis was repositioned but eventually dislocated again, highlighting the complexities of managing such advanced injuries in older patients.
Case 5: 46-year-old male, athlete
A 46-year-old athlete with a comminuted coronoid fracture and severely damaged radial head required multiple surgeries after an overstuffed radial head prosthesis caused complications. The final solution was a total elbow prosthesis, underscoring the importance of careful prosthesis sizing and ligament repair.
In conclusion, while conservative treatment might be an option for some terrible triad cases, careful attention to radial column stability, ligament repair, and coronoid fixation is critical to achieving a durable result. Early mobilization and a well-executed repair plan are key to a successful recovery. Special attention should be paid to:
- Concentric joint reduction is crucial for a stable elbow joint.
- Radial column stability is essential; avoid any issues with pronation-supination.
- Evaluate the coronoid—is it just the tip or a more extensive fracture?
- Aim for a stable range of motion (30-40° flexion is acceptable) to avoid subluxation.
References and further reading:
- O'Driscoll SW, Jupiter JB, Cohen MS, Ring D, McKee MD. Difficult elbow fractures: pearls and pitfalls. Instr Course Lect 2003;52:113-34.
- Beingessner DM, Stacpoole RA, Dunning CE, Johnson JA, King GJ. The effect of suture fixation of type I coronoid fractures on the kinematics and stability of the elbow with and without medial collateral ligament repair. J Shoulder Elbow Surg. 2007 Mar-Apr;16(2):213-7. doi: 10.1016/j.jse.2006.06.015. PMID: 17399625.
You might also be interested in:

AO Trauma shoulder and elbow courses
Learn the current management of patient pain, dysfunction, deformity, and cosmesis related to trauma of the shoulder and elbow.

AO Trauma videos
Explore the vast collection of first-class videos and expert presentations by leading AO Trauma surgeons.

AO Trauma Guest Blog
Advancing trauma care, one story at a time, by showcasing diverse voices and perspectives from our community.