

Incidental lumbar durotomy—accidental tears in the dura mater that result in leakage of cerebral spinal fluid (part 1)
About the article: This article is part of a series of twelve posts that aim to present key points of these less formal expert conversations. The goal is to convey the key points in the surgeons’ own words. The articles can be read on their own or used as a supplement when viewing the recordings.
Download the related White Paper on Accidental tears in the dura mater that result in leakage of cerebral spinal fluid (June 2020).
Speakers are identified first by their full name and then by their initials. The corresponding time in the video is included in parentheses.
Watch a recording of the full discussion here:
Incidental durotomy, resulting in cerebral spinal fluid leakage
Incidental durotomy (ID), resulting in cerebral spinal fluid (CSF) leakage, is one of the most common and often challenging complications in spine surgery. The incidence varies widely, ranging from 1% to 17%, depending on the location in the spine and type of procedure. Revision surgeries present almost twice the risk of CSF leakage as primary surgery. Meticulous decompression and regular use of a microscope probably reduce ID in the cervical spine when compared with the lumbar spine.
Some types of lumbar pathologies have a higher chance of ID, such as spondylolisthesis, spinal stenosis, and, in particular, synovial cyst. ID can be twice as frequent in open lumbar surgery, especially in revision cases, compared to minimally invasive surgery (MIS). The prevalence of ID in surgery involving anterior or lateral access is around 2% and can be as high as 37% in full endoscopic treatment of synovial cysts.
A gold standard for management of intraoperative and postoperative cerebrospinal fluid leakage is still lacking in the literature. A survey of German, Austrian, and Swiss spine surgeons showed that isolated bed rest, simple suture, use of fibrin sealant patch and fibrin glue were all treatment strategies. In that study, most surgeons prescribed 24 to 48 hours postoperative bed rest. Another survey conducted in Germany showed no consensus regarding the treatment of incidental durotomy. Considering the different approaches to the lumbar spine, ID management should be individualized.
The objective of the AO Spine Clinical Expert Advice group (White Paper and webinar) is to describe the stepwise treatment of intraoperative ID by expert spine surgeons from five continents for four clinical scenarios.
Impact on morbidity and health costs
The consequences of a non-identified durotomy can be devastating, with complications including infection, pseudo meningocele, meningitis, radiculopathy, caudal displacement of intracranial content, and subdural hematoma. A retrospective analysis of hospital costs for elderly patients who underwent discectomy with ID complication showed an increase of over USD 4'000.
Asdrubal Falavigna (AF) began the webinar on “Accidental tears in the dura mater that result in leakage of cerebral spinal fluid” by using detailed slides (4:30) to discuss the impact of incidental durotomy (ID) on morbidity and health costs.
AF (7:20): The take home message is that in this situation, there is little evidence in the literature. The patient has high expectations. The surgeon’s experience is the main and the only option. In the end, prompt recognition and meticulous repair are the solutions.
Dangerous procedures that can result in incidental durotomy
Yoshiharu Kawaguchi (YK) presented several videos from posterior lumbar surgery (8:00) that included ID.
YK (8:25): 73-year-old male with L5 isthmic spondylolisthesis. The surgeon is making fenestration of L4/L5 using high speed burr. The tip of the burr is steel. Upper is medial, lower is lateral. You can see incidental durotomy. What will you do? Don’t get upset! That is very important. The doctor will confirm the hole; the hole is very small. Fortunately, the doctor can suture the hole. This frequently happens.
YK (9:30): There are two types of burr tips: steel burr and diamond burr. Steel tip is dangerous, with the potential for direct injury. So be very careful! Diamond tip is relatively safe, but heat injuries might occur.
YK (10:00): 77-year-old female, with L4/5 degenerative spondylolisthesis. You must be aware that using rongeurs for spondylolisthesis are very dangerous. When the surgeon uses a rongeur, a weak grip is OK, but a tight grip causes incidental durotomy. As in this case, when the ligamentum flavum is removed with a tight grip.
YK (11:05): 63-year-old man, with lumbar canal stenosis (LCS) re-decompression. Also here, rongeurs for the reoperation are dangerous. You can see incidental durotomy occur. The surgeon tried to make a bigger hole and tried to insert Vycril wire into the dura. However, it is very difficult because the hole is so small. So, the surgeon tried to make a bigger hole with the diamond burr and cut the dura. Tried to insert Vycril wire into the dura. Tried to clip. However, this case, it is very dangerous. It is impossible, so the surgeon tried to use artificial dura mater.
YK (13:05): 60-year-old man, F4/5 degenerative spondylolisthesis. You can see malposition of the pedicle screw. The surgeon tried to remove the pedicle screw and to remove the small bone tip. The surgeon confirms the small hole around the nerve root. You can see the small hole and the nerve filament from the nerve root. So, the surgeon tries to confirm that hole. Fortunately, the hole is small, so he can suture the hole. The surgeon tried to suture with 6/0 nylon braid. Fortunately, this is a very small hole, so he used polyethylene glycol and fibrin glue in packing, and fat graft. Then fibrin glue again, and bigger fat graft.

Intraoperative incidental durotomy during lateral (LLAF) or anterior (ALIF) approach
Lateral and anterior approaches are becoming very common. They are becoming the preferred approaches for many spine surgeons to restore sagittal alignment and to get good anterior fixation. Néstor Taboada (NT) presented detailed slides (17:20) on a typical clinical case.
NT (21:15): In our service, we perform 150 anterior and lateral approaches per year, and three incidental durotomies have been presented in the last 10 years. We suggest bed rest of only 24 hours. It was not necessary to review any of the three cases in our experience. In our initial case, after the incidental durotomy, the deambulation began the next day, and the patient did not present symptoms of dural tears. In conclusion, incidental durotomy in anterior lumbar approach has had very low incidence.
Avelino Parajón (AP) (22:25): So, the most frequent and arduous complications in the anterior and lateral approaches, we can say they are not durotomies. In recent reviews for example in the British Journal of Neurosurgery, the incidence of dural tears in ALIF was only one case in a total of 241 cases. However, there are some publications [...] where the incidence can be as high as 10%. So, surgeons, we must be aware and know how to solve them.
AP (23:10): In lateral transpsoas approaches—or prepsoas—also the probability of having a dural tear is very low. But in some cases, it can be cumbersome. For example, in the thoracic spine, we are doing more and more lateral approaches. In the thoracic spine—a dural tear—if it’s not well repaired, it can cause CSF collection in the pulmonary cavity, and this can be a huge problem. In many cases you need a reintervention.
Michael Wang (MW) (24:10): What we are seeing here is a new technology, which is the lateral approach and of course the anterior approach is already being used. But when you look at this type of problem, this is a very difficult case and I think the surgeons here handled it very well. This is a very, very interesting area where we have to find new techniques to close the dura. And I think that one of the values of the AO webinars is to be able to see how people are doing this and managing the new complications that we have arrived at.

Pure endoscopic surgery
MW (25:00): There has been a lot of development in pure endoscopic surgery in recent times. The concept of pure endoscopic surgery is relatively new area in America, but in Asia and for example in Germany this has already been very popular.
MW (25:35): The video shows the case of an interlaminar approach, and this type of interlaminar approach is being used with a slightly larger working channel, this is called a Delta system. It’s a 1 cm diameter, so it’s a little bit bigger than the standard interlaminar method.
MW (25:50): We’re doing a case of very tight stenosis and we’re drilling and removing bone in the lamina and then later on in the ligament. This is a totally different type of setting. If you’ve never used this technology, the reality is you only really get one working portal. In other words, you don’t get to use two different sets of instruments. At any one time, you only have the one instrument.
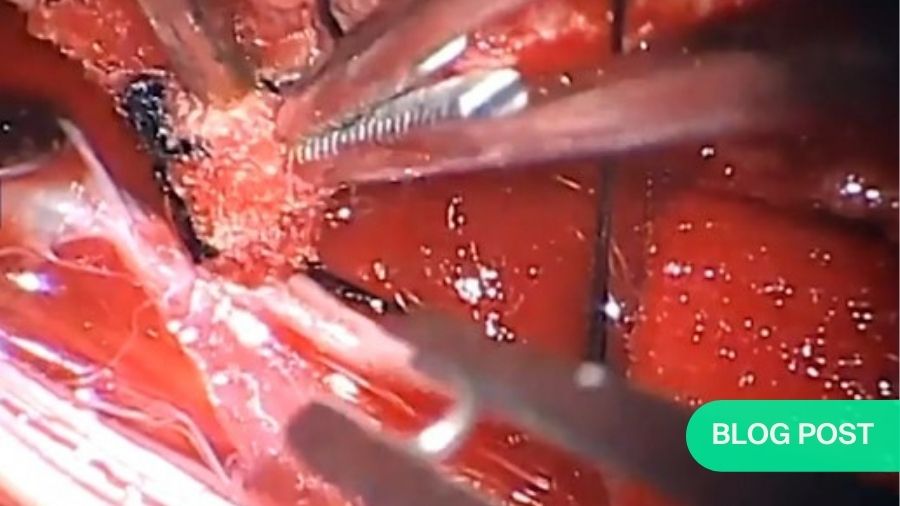
MW (26:10): So, we have to switch—for example—between drilling to thin out the lamina, and now we’re going to use the Kerrison to try and take the remainder of the bone. You see us going back and forth [...] In reality it should happen just like a standard open or mini-open type of surgery. The surgery proceeds. And this is a case where there is very tight stenosis, and we arrive at an area where there is no ligamentum. Here you can see, this is a very interesting point. We’ve become so reliant on using the irrigation pressure to keep the dura away from us, that we inadvertently bite the dura. There, you can see it right there. Not only do we bite the dura, but there’s also actually a neural injury. You can see that some of the nerve—which in essence wasn’t clinically relevant—was actually lacerated by that.
MW (27:05): This is a very, very stressful situation, because you cannot simply go in and sew this up. I’ll be curious to see how the panelists feel about this. Should you convert this surgery to open? [...] Now we’re forced to try to work around this. This is very aggravating. We’re now starting to work our decompression. We’ve rotated the endoscope to look laterally. And if you haven’t done these surgeries, it is a little bit disorienting.
MW (27:45): We’re going to continue all of that with these rootlets in your way. Again, there’s no way to sort of push this stuff out of the way actively. Even if you put a cottonoid or a patty there, every time you put an instrument in or out, they’re fitted almost exactly to the bore size. So, you’ll pull your cottonoid in and out and in and out. It’s actually a little bit difficult to handle this. But you have to keep your cool. We’re going to go laterally, then we’re going to do the cranial and caudal decompression. So, we’re trying to finish the laminar decompression despite the presence of those rootlets.
MW (28:20): In this particular case, I believe a major culprit was the loss of irrigation pressure. At one point, the whole irrigation had run out. So, there was no positive pressure depressing upon the dura.
MW (28:40): And then the question arises, how do you really repair this? I think this is a point of discussion. When you’re doing the very small approaches, whether it be using a 14mm tube or a 16mm tube. Or in this case, a 10mm tube. Do you need to primarily repair this? Do you need to sew this back up? Or can you simply rely on the soft tissue not been so disrupted to prevent you from having a pseudomeningocele, or sort of a permanent CSF leak.
MW (29:05): In this case, what we decided was to put down DuraGen, which is a collagen matrix. I think we’re going to see some interesting discussion later on about how to patch the dura. We place that (the DuraGen) and then use a fibrin glue to patch that up, and then rely on the soft tissue to envelop the tissue.
Final questions:
Can you repair the area of the incidental durotomy, using a small hole?
MW (30:25): With existing technology, the only technology I’m aware of that might work is a nitinol clip, that is a self-closing clip that you may be able to fit through the endoscope. The problem is that I think even that is too big to fit through most of these endoscopes. The second part is […] usually we can push the nerve roots away then sew. But in endoscopy, you cannot push the nerve roots away and clip or sew, because you can only put one instrument through. So, this is a very interesting area of exploration. Maybe you can put a barrier first to keep the nerve roots away and then clip it?
YK (31:15): How about using a polyethylene glycol sheet?
MW (31:20): In this case we used a collagen sheet and fibrin glue [...] But somehow you have to mechanically sew it, and that’s the hard part. Maybe you can put a sheet down, then staple it in place over everything. There are some new glues being developed. Maybe you can put a glue and then a sheet. I don’t know if you can do that through an endoscope. Everything is hard through an endoscope.
YK (31:55): I always use a polyethylene glycol sheet and fibrin glue.
What are the dural tears you can leave without suture?
MW (32:25): I think the reality is every time we encounter this, we don’t know what’s going to happen. You’re making a statistical prediction. Some people err on the side of being more aggressive to stop the CSF leak [...] There will be cases where you didn’t repair the dura and it’s OK. And there are going to be other cases where you didn’t repair the dura and you’re going back to surgery. Ultimately, the surgeon’s philosophy plays the big part. If you can repair it, we always try to do that.
MW (33:20): In this particular case, the question was, if we were willing to convert the surgery to an open operation in order to achieve that. In that case we did not. But that doesn’t always work.
YK (33:30): I agree with Michael [...] Lumbar drainage is very effective. Especially with liquid discharge from the cervical and the thoracic spine. From the cases with ossification of the posterior longitudinal ligament (OPLL), we always use lumbar drainage.
SR (33:55): We always hear of this term “watertight closure”. Many of the neurosurgeons talk of “OK, if you have a pinhole dural tear then it’s important to repair it. But if you have a bigger dural tear then it’s not [...] The CSL will look after itself, just do a watertight closure. How much do you believe in this term “watertight closure”? Does it work?
MW (34:25): I don’t know if that’s really true, because it depends on how much pressure there is, right? Then it depends on healing. Ultimately, it’s a race of healing. The healing has to happen. You bring up a very important point. Maybe for some of the younger surgeons, they are not aware that the small tears are the really bad ones. The giant tears, when you’re doing an open surgery, somehow those people end up healing. Whether it’s an inflammatory reaction, blood in the area, whatever. It’s the lumbar microdiscectomies that are so annoying. Those are the ones that really come back again and again.
What do you think of bone scalpels and ultrasound instruments which are supposed to cause less injury to the dura?
YK (35:30): I sometimes use ultrasound instruments. Especially for cutting LBLL, that is very effective. However, the speed is very, very low. So, I prefer to use a diamond burr—usually.
The Clinical Expert Advice Forum discussion on Incidental lumbar durotomy continues here. Part 2 covers MIS TLIF—minimally invasive transforaminal lumbar interbody fusion, Dural sealants, Reasons for postoperative CSF leakage unnoticed intraoperatively, the role of best rest, lumbar drainage, and prophylactic antibiotics, Closed CSF collection—symptomatic and asymptomatic.
Download the White Paper on Accidental tears in the dura mater that result in leakage of cerebral spinal fluid (June 2020).
Find more Clinical Expert Advice Forums titles here.
About the authors:
The AO Spine Clinical Expert Advice Forums address clinical situations where clinicians can benefit richly from the experience of experts, but rigorous scientific research may not be possible. These forum rounds resulted in six White Papers and webinars in 2020 –2021. The webinars include detailed slides to support the conversations.
The Clinical Expert Advice Forum for “Incidental lumbar durotomy" are Asdrubal Falavigna (Brazil), André Castilho (Brazil), Yoshiharu Kawaguchi (Japan), Bastian Storzer (Germany), Karsten Wiechert (Germany), Nestor Taboada (Colombia), Jason Ilias Liounakos (USA), Michael Yung-Shun Wang (USA), Avelino Parajón (Spain), and S. Rajasekaran (India).