

Cervical sagittal alignment: why ACDF should be planned as a global intervention
BY DR MARCO MANZETTI

Cervical spine surgery should be planned as a global alignment intervention rather than a purely segmental fix. Drawing on one of the largest radiographic analyses of multilevel ACDF to date, I will explain why I think alignment matters, how compensatory mechanisms develop, and what we as surgeons can change through preoperative planning. It is time to shift the focus from simple decompression to the shape, balance, and long-term biomechanical health of the cervical spine.
-
Read the quick summary:
- Spine surgeon Marco Manzetti explains why ACDF should be planned as a global cervical alignment intervention, not a segmental decompression.
- Multilevel ACDF can reverse compensatory mechanisms and improve global cervical balance when lordosis is restored.
- Surgeons should use lateral radiographs and alignment metrics to plan ACDF shape, not just levels and decompression.
- Linking alignment correction to patient-reported outcomes and long-term adjacent segment health remains ongoing.
Disclaimer: The article represents the opinion of individual authors exclusively and not necessarily the opinion of AO or its clinical specialties.
How is ACDF traditionally approached in cervical spine surgery?
For many spine surgeons, anterior cervical discectomy and fusion (ACDF) is one of the most familiar and reliable procedures, where decompression of neural structures and achievement of a solid fusion are often seen as the primary goal.
However, our understanding of spinal biomechanics has evolved. In the thoracolumbar region, it has become clear that how we fuse matters just as much as where we fuse. During my AO Spine fellowship at Schulthess Klinik, working under the mentorship of Markus Loibl, one question came into my mind—why do we treat cervical degeneration as a local problem, when it behaves as a global alignment disorder?
Why fusion position matters biomechanically
Most operations we perform for degenerative conditions involve fusion: we stabilize diseased segments, but in doing so we remove motion at those levels. That makes the final position in which you “lock” those segments crucial—not only because it cannot be changed spontaneously afterwards, but also because it influences how the remaining healthy, mobile segments behave once the patient upright.
Therefore, good alignment is important not only to treat the pathological segment, but also to avoid forcing healthy segments into chronic compensation.
How do compensatory mechanisms develop in the cervical spine?
At first, compensations can be helpful: they keep the gaze level quickly. The problem is that they shift load and motion to segments that are not meant to work that hard for that long, especially the upper cervical region, which may remain in extension.
This increases stress on facet joints, capsules, ligaments, and muscles, and it concentrates motion into the few levels that remain free.
With a fusion, the effect becomes even clearer: adjacent levels become the main remaining “hinges,” so they tend to develop hypermobility and overload. Over time, a vicious cycle can develop: more compensation leads to more stress, then more degeneration and stiffness, which in turn increases the need to compensate –potentially extending the problem to segments that were initially healthy.
What does radiographic evidence show after multilevel ACDF?
Our recent study, published in the European Spine Journal, explored how multilevel ACDF affects cervical sagittal alignment and the compensatory mechanisms that patients develop to keep their head balanced and their gaze horizontal. (You can read the full study here.)
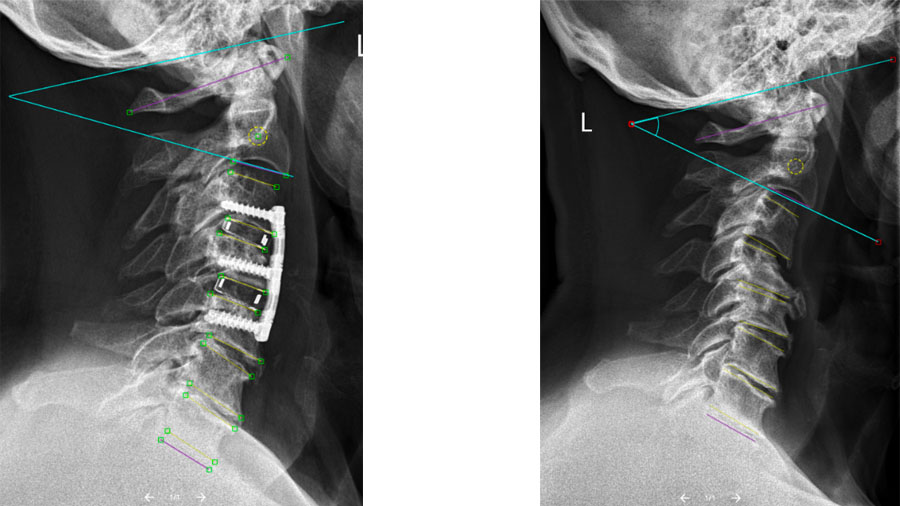
The study itself was a retrospective radiographic analysis of 290 patients with cervical spondylosis who underwent two- or three-level ACDF, with a minimum of one year of follow-up. Using an image-analysis system, thousands of pre- and postoperative lateral cervical radiographs were assessed to quantify key sagittal alignment parameters. These included:
- Subaxial cervical lordosis (C2–C7)
- Upper cervical lordosis (C0–C2)
- Surgical and unfused segment lordosis
- T1 slope
- Cervical sagittal vertical axis
How does lordosis restoration affect global cervical alignment?
This large dataset—comprising thousands of radiographic images—allowed us to examine how changes achieved at the fused segments related to alignment changes elsewhere in the cervical spine. The analysis showed that improvements in surgical and subaxial lordosis were strongly associated with a reduction of compensatory hyperextension in the upper cervical spine and unfused segments. This supports the concept that multilevel ACDF can induce a system-wide realignment within the spine rather than acting as a purely local intervention in the neck.
These findings matter for everyday clinical practice and hopefully they can inform a more thoughtful, systems-based approach to cervical spine surgery.
From decompression to alignment: a shift in perspective
Degenerative cervical disease is traditionally approached through the lens of symptoms such as neck pain, radiculopathy (nerve root compression causing radiating arm pain with numbness/tingling or weakness), and myelopathy (spinal cord compression causing clumsiness, gait imbalance, and broader weakness or sensory changes).
Imaging often reinforces this focus—MRI highlights disc herniations, osteophytes, and spinal cord compression. Logically the surgical solution would be to remove the offending pathology and stabilize the segment.
But the cervical spine does not function in isolation. It supports the head, maintains horizontal gaze, and allows a remarkable degree of motion—all while sitting atop the thoracic and lumbar spine. When degeneration alters its shape, the entire body responds immediately.
What preoperative postures indicate cervical compensation?
During my fellowship, I noticed that patients undergoing multilevel ACDF often presented with certain preoperative postures: chin elevation, hyperextension at adjacent levels, or a rigid upper cervical spine. These features were not random. They were compensatory mechanisms working to keep the head centered despite an inefficient or kyphotic subaxial spine.
The key question then became: if we correct the alignment where the pathology is, will the rest of the cervical spine stop compensating?
Compensation: the body’s pragmatic solution
The spine behaves much like a structural column. Its efficiency depends on alignment. When one segment loses its optimal shape, other segments within the system adapt.
In the cervical spine, the overriding goal is simple: keep the head level and the eyes facing forward. If degenerative changes flatten or reverse lordosis in the mid-cervical region, the body recruits other segments to do the work resulting in:
- Upper cervical extension (C0–C2) to “lift the chin”
- Hyperlordosis of unfused subaxial segments
- Adjustments extending into the cervicothoracic junction and beyond.
While these adaptations initially help by restoring balance quickly, over time they can cause other problems.
Why prolonged compensation becomes harmful
The upper cervical spine is highly mobile but not designed to remain in end-range extension for years. Facet joints, ligaments, suboccipital muscles, and capsules are subjected to sustained stress. When fusion is added to the mix, the remaining mobile segments become the primary hinges, concentrating motion and load where the tissue may already be vulnerable.
This is the biomechanical backdrop against which ACDF is performed—and it explains why alignment should not be an afterthought.
Why multilevel ACDF changes the equation
Single-level ACDF rarely produces major changes in global alignment. Its impact is often local, and compensatory mechanisms are usually minimal. Multilevel ACDF is different.
When two or three levels are fused, a substantial portion of subaxial mobility is removed, segmental lordosis can be altered, and the overall cervical curve, as well as the head position, can change.
This makes multilevel ACDF a powerful intervention, not just for decompression, but for realignment. It also makes planning more consequential: the shape you create is the shape the patient will live with.
Our analysis showed that the number or exact location of fused levels mattered less than the quality of correction achieved. When lordosis was restored at the operated segments, the rest of the cervical spine consistently responded.
What happens to cervical balance after alignment correction?
One of the most striking observations from our work was how the cervical spine relaxes after favorable correction.
When segmental and subaxial lordosis are restored, upper cervical hyperextension decreases, unfused subaxial segments reduce their compensatory lordosis and overall sagittal balance improves.
In other words, correcting the inefficient segment reduces the need for the system to compensate elsewhere. This finding has important clinical implications. The cranio-cervical junction is often where patients report stiffness, fatigue, and muscular pain. Allowing this region to operate within a more physiological range may reduce chronic overload, even if this benefit is not immediately captured by standard outcome scores.
The cervical spine as a system
A recurring theme in our analysis was that many radiographic “abnormalities” above and below the diseased segment were not primary problems. They were responses to the primary problem. After surgery, when alignment improved, these responses often diminished. This suggests that:
- Hyperlordosis at adjacent levels may reflect compensation, not degeneration
- Upper cervical extension is frequently secondary, not intrinsic pathology.
This system-based view mirrors what already happens in lumbar spine surgery, where global sagittal balance has become central to planning. The cervical spine deserves the same consideration.
How should surgeons plan ACDF using alignment principles?
So, what does this mean for surgeons planning ACDF? It suggests a shift from asking only, “Which levels should I fuse?” to also asking:
- What is the global cervical alignment?
- Where is the patient compensating?
- What shape am I reconstructing?
Practical considerations include:
- Careful assessment of lateral radiographs, not just MRI
- Evaluation of C0–C2 posture and adjacent segment lordosis
- Consideration of T1 slope as a bridge between cervical and global alignment
- Selection of implants and techniques with lordosis restoration in mind
Importantly, compensatory changes should not automatically be labeled as pathology requiring treatment. Instead, they can be viewed as markers of how severe and inefficient the primary deformity has become.
How does cervical alignment influence postoperative neck pain?
Do these findings mean that unresolved alignment causes postoperative pain? In some cases, yes, but not exclusively.
Postoperative neck pain has many causes: infection, subsidence, residual compression, pseudarthrosis, or hardware-related issues must always be excluded first. Alignment should be seen as only one piece of the puzzle.
If a patient is fused in an unfavorable position, the remaining segments may continue to compensate, leading to muscular fatigue, stiffness, and discomfort despite adequate decompression. In such cases, alignment analysis can provide a biomechanical explanation when other causes are ruled out.
The key message is not that every ACDF must achieve perfect lordosis, nor that alignment trumps decompression. Rather, it is that ACDF has the potential to reorganize cervical balance, and whether it does so favorably depends on surgical planning.
Our data suggests that:
- The cervical spine responds globally to local correction
- Compensations are often reversible
- Quality of correction matters more than construct configuration
Recognizing these principles allows surgeons to use ACDF not just as a stabilizing procedure, but as a tool to reduce biomechanical stress across the cervical spine.
What are the next research questions in cervical sagittal alignment?
Moving forward, the next step should be to link radiographic information to patient-reported outcomes, long-term function, and adjacent segment health. Understanding who benefits most from alignment correction—and why—will make these concepts even more actionable.
For now, the takeaway is simple—cervical spine surgery should be planned as a global alignment intervention, not an isolated segmental surgery. By recognizing compensatory mechanisms and aiming to reconstruct a favorable cervical shape, we can reduce the need for chronic compensation and potentially improve the long-term biomechanical environment of the neck.
About the author:

Marco Manzetti, MD, is an orthopedic surgeon at IRCCS Istituto Ortopedico Rizzoli (Bologna, Italy), with a clinical and research focus on spine surgery and sagittal alignment. He completed his residency in Orthopedics and Traumatology at IRCCS Istituto Ortopedico Rizzoli and is currently a PhD candidate in Biomedical and Neuromotor Sciences at the University of Bologna. He trained internationally through fellowships at Schulthess Klinik Zurich (AO Spine, Prof Markus Loibl) through the AO Spine Fellowship Program and at CHU Bordeaux (Sagittal Balance and Spinal Deformity, Prof Jean-Charles Le Huec). He has multiple peer-reviewed publications and serves as a peer-reviewer for the Global Spine Journal, where he has received recognition and been acknowledged as the ”Top Reviewer of the Month” for December 2025.
The author would also like to acknowledge the contributions of Prof Markus Loibl (Schulthess Klinik, Zurich), Dr Fabio Galbusera (Schulthess Klinik, Zurich), Dr Andrea Cina (Schulthess Klinik, Zurich), Dr Tamás Fekete (Schulthess Klinik, Zurich), Prof Alberto Ruffilli (IRCCS Istituto Ortopedico Rizzoli), and Prof Cesare Faldini (IRCCS Istituto Ortopedico Rizzoli).
Further reading:
You might also be interested in...

AO Spine fellowship
The AO Spine Fellowship Program offers a unique educational experience to the most promising young surgeons in the entire field of spine surgery.

Global Spine Journal
The official scientific publication of AO Spine, peer-reviewed open access GSJ is devoted to the study and treatment of spinal disorders.

AO Spine Education
From face-to-face practical courses to recorded webinars, AO Spine has the educational options to help you enhance your skills and build your career.