

How useful are scoliosis exercises for adolescent patients with idiopathic scoliosis?
BY DR EMRE ACAROGLU

I had the opportunity to rethink the usefulness of the Schroth Method exercises based on a recent scientific publication. As those of us who are interested in the subject—whether physicians or those with living with or caring for people with scoliosis—know, the Schroth Method is an exercise program to correct or at least to stop the progression of scoliosis. The method was first defined almost half a century ago. I remember being very skeptical of the method in the past, main reason being the lack of sufficient and high-quality scientific evidence on the subject. Now, I could finally see some reliable evidence to evaluate the method and wanted to review my position.
Disclaimer: The article represents the opinion of individual authors exclusively and not necessarily the opinion of AO or its clinical specialties.
Numerous earlier studies have supported the efficacy of the Schroth Method. Research indicated that patients who stringently followed Schroth exercises showed significant improvements in posture, pain levels, and overall function in fairly short follow-up periods. While some medical professionals remained cautious about its ability to reduce spinal curvature—the author of this post included—the method has become widely utilized as a stand-alone treatment or a component of a comprehensive scoliosis management plan.
The 50-year journey of scoliosis exercises
Scoliosis, a lateral curvature of the spine, affects many individuals, particularly adolescents. Adolescent Idiopathic Scoliosis (AIS) with no known cause is the most common form of scoliosis. Over the past 50 years, various exercises and physical therapy programs have been prescribed to manage this condition.
In the 1970s, scoliosis management primarily focused on bracing and surgery, with exercises playing a supplementary role. The exercises aimed to improve general spinal health and support bracing but were not seen as a standalone treatment. Physical therapy focused on stretching and strengthening the back muscles, enhancing flexibility, and reducing discomfort.
By the 1980s and 1990s, the Schroth Method emerged, with the premise revolutionize scoliosis treatment. Developed by Katharina Schroth in Germany, this method emphasized specific exercises tailored to the three-dimensional nature of scoliosis. These exercises aimed to de-rotate, elongate, and stabilize the spine, offering a more targeted approach.
The early 2000s saw further advancements with the integration of core stabilization exercises. Techniques such as Pilates and yoga were incorporated, focusing on overall body alignment, core strength, and improved posture. This holistic approach aimed to manage scoliosis more effectively by addressing the entire musculoskeletal system.
Debate around non-invasive treatment for scoliosis
Today, there is a greater emphasis on non-surgical treatments for AIS, and exercise programs are attained a significant role. The common impression among many practitioners is that exercises— particularly those rooted in the above mentioned Schroth Method—can help manage scoliosis by improving muscle balance, enhancing posture, and potentially reducing curve progression. However, this is not without controversy.
Support for scoliosis exercises:
- Schroth Method: Numerous studies have shown that the Schroth exercises can improve the quality of life and reduce pain for individuals with scoliosis (in short term). They are designed to be patient-specific, addressing individual curve patterns. But as mentioned earlier, the studies are lacking long-term follow up for stronger evidence.
- Core stabilization and Pilates: These exercises focus on strengthening the core muscles, which support the spine and improve overall posture. Evidence suggests they can enhance functional outcomes and are beneficial as part of a comprehensive treatment plan especially in kyphotic patients.
- Yoga: Incorporating flexibility and strength exercises, yoga can improve overall spinal health and is recommended by some practitioners as a complementary therapy.
Controversies around scoliosis exercises
- Lack of standardization: One major controversy is the lack of standardized protocols across different exercise programs. This variability makes it challenging to compare outcomes and establish evidence-based guidelines.
- Limited evidence on curve reduction: While exercises can improve symptoms and functional outcomes, their effectiveness in reducing spinal curvature remains questionable. Some studies suggest minimal impact on the curve itself, leading to skepticism among some medical professionals. In addition, almost all studies reporting beneficial results regarding curve correction (or maintenance) have very short (3 to 6 months) follow-up periods. We practically do not know what happens to these patients over longer periods.
- Patient adherence: The success of exercise programs largely depends on patient adherence for extended periods. Given that these exercises are often quite stringent (please refer to the exercise regimen included below) and require long-term commitment, maintaining motivation can be challenging, particularly for adolescents.
Looking at the effectiveness of scoliosis exercises through the evidence
Although there have already been numerous papers published on the topic of Schroth exercises and adolescent idiopathic scoliosis (AIS) over the years, and although they often reported successful results, the patient follow-up periods were commonly very short. Even a six-month follow-up was rare.
Now, thanks to a recent meta-analysis published in the journal Spine Deformity, we finally have a high-quality publication on the subject: The impact of patient scoliosis-specific exercises for adolescent idiopathic scoliosis: a systematic review and meta-analysis of randomized controlled trials with subgroup analysis using observational studies.
But before moving on to the results, let me briefly explain the method.
A 'meta-analysis' collects all the studies published on a subject in the literature so far, classifies them according to their quality and eliminates those that are not of appropriate quality. In this case, only 26 out of a total of 628 publications with 2083 patients met the quality standards.
You then blend the data and results of the publications and analyze them in a single data set.
Thus, a large database is created, which makes it possible to reach a high level of evidence from the sum of publications, each of which may not constitute perfect evidence on their own. In fact, in this case, the journal gave the Level of Evidence of this publication as 1 (one). Absolutely reliable.
In summary, the recent study concludes that considering the publications in the control group—i.e. some of the patients exercised, others did not, and these two groups were compared—the scoliosis measurements of the patients who exercised after an average of 14.5 +/- 20.0 months (which means approximately a few months to a few years later) were found to be 2.5 degrees less than those who did not.
Let me repeat: two and a half degrees. At this point, you should note that the margin of error of scoliosis measurements is +/- 4 degrees.
In addition, no difference was found in the patients' vertebral rotations, i.e., torsion of the spine that causes a protrusion in the back, and clinical scores. So basically, no real differences to speak of.
Regarding the Schroth Method, let me revisit my original question: should we continue to expose our patients or children to this grueling and stressful practice, knowing that it will provide corrections within the measurement margin of error, 2.5 degrees on average?
What do you think?
Towards a more personalized holistic treatment
The future likely holds further research and refinement of supplementary techniques, aiming to provide clearer guidelines and improve outcomes for those with AIS. As we in the medical community continue to explore and validate these approaches, the hope is to offer effective non-invasive options for managing scoliosis. The quest to offer valid and effective treatments will continue.
A blog post by Emre Acaroğlu on the usefulness of the Schroth Method was published in Turkish in May 2024 here.
About the author:

The Schroth Method
The Schroth Method is a form of physical therapy designed for scoliosis patients. Developed by Katharina Schroth in the 1920s in Germany, it has since gained significant recognition, especially for its application in Adolescent Idiopathic Scoliosis (AIS).
The Schroth Method aims to treat the three-dimensional aspects of scoliosis through customized exercises that focus on elongating and de-rotating the spine, aiming to improve posture and reduce curvature, not only the sideways but also the rotational and sagittal plane deformity of scoliosis.
The method incorporates a combination of breathing techniques, postural training, and specific exercises to address these complexities. Each patient undergoes a thorough assessment to determine their specific scoliosis curve pattern. This includes identifying the primary and secondary curves, the degree of rotation, and the impact on posture and overall spinal alignment.
1. Customized exercise regimen: Based on the assessment, a tailored exercise program is developed for the patient. These exercises are designed to:
- De-rotate the spine: Exercises target the rotational aspect of scoliosis, aiming to reduce the twisting of the spine.
- Elongate the spine: Techniques to stretch and lengthen the spine help counteract the compressive forces of the curves.
- Stabilize the spine: Strengthening exercises focus on core muscles and the muscles supporting the spine, providing better stability and support.
2. Breathing techniques: A crucial component of the Schroth Method is the use of specific breathing techniques known as Rotational Angular Breathing (RAB). These techniques encourage patients to breathe into the concave side of the torso, helping to expand and derotate the spine. This also improves lung function and overall respiratory health, which can be compromised in severe scoliosis cases.
3. Postural training: Patients are taught how to correct their posture in daily activities. This includes training in sitting, standing, and walking postures that promote spinal alignment and reduce asymmetrical loading on the spine.
The method is aimed to reduce by addressing muscle imbalances and improving posture, the method helps reduce pain associated with scoliosis. Improved posture is to be achieved with customized exercises that help patients achieve a more balanced and aligned posture, which can improve overall appearance and self-esteem.
The outcome from the exercise regime is lead to enhanced quality of life. As patients experience better physical function, it allows them to participate more fully in daily activities and sports. While the method may not drastically reduce the curvature in all cases, it can help prevent further progression, particularly during growth spurts in adolescents.
The "side-shifting" exercise—an example from the Schroth Method
A common Schroth exercise is the "side-shifting" exercise, which aims to correct the lateral curvature of the spine by focusing on muscle strengthening and elongation.
Steps to perform the side-shifting exercise:
1. Starting Position:
- Stand with feet shoulder-width apart.
- Place your hands on your hips to help maintain balance.
2. Side shift:
- Shift your hips towards the convex (curved outward) side of your scoliosis curve.
- At the same time, lean your upper body towards the concave (curved inward) side.
- This creates an active elongation of the spine and engages the muscles on the convex side to contract.
3. Rotational breathing:
- Incorporate rotational angular breathing by deeply inhaling into the concave side of your torso.
- Focus on expanding the ribs and stretching the intercostal muscles (muscles between the ribs).
4. Hold and repeat:
- Hold this position for a few seconds while maintaining deep, controlled breaths.
- Return to the starting position and repeat the exercise several times, as recommended by your therapist.
This exercise aims to help balance muscle activity, elongate the spine, and improve postural alignment. It's typically performed under the guidance of a trained therapist to ensure proper technique and maximize benefits.
The Schroth Method has been seen as a significant advancement in the non-surgical treatment of scoliosis. By addressing the three-dimensional nature of the condition through personalized exercises, breathing techniques, and postural training, it offers a holistic approach to managing AIS. But as the latest studies show, research and further validation of methods must continue to find effective options for improving the lives of those living with scoliosis.
You might also be interested in:

AO Spine Deformity Courses
Find all upcoming AO Spine deformity courses and events in your region, including simulation and specimen courses, and our upcoming flagship AO Davos Courses.
AO Spine Knowledge Forum Deformity
AO Spine sponsors innovative studies in the field of spinal deformities, generating and translating new knowledge that matters to our members and to our patients.
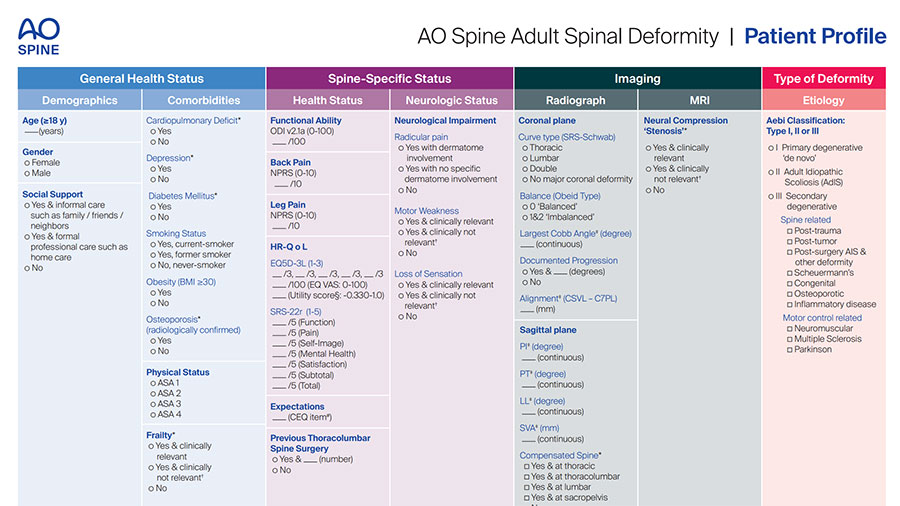
AO ASD Patient Profile
Optimize your treatment of Adult Spinal Deformity (ASD) with our comprehensive patient evaluation tool, the AO Spine ASD Patient Profile, designed for clinical practice and training.