
Pastern Arthrodesis in the horse: Current controversies
BY DRS JEFFREY P. WATKINS AND KATI GLASS

Locking compression plate arthrodesis remains the gold standard for pastern fusion in horses, offering reliable outcomes and low complication rates. While minimally invasive and ligament-sparing techniques show promise, current evidence supports the standard open approach for most cases. This blog article reviews technique selection, addresses ongoing debates, and offers practical guidance for optimizing outcomes.
-
Read the quick summary:
- Drs Jeffrey P Watkins and Kati Glass review the evolution of pastern arthrodesis techniques in horses, highlighting current debates about standard vs. minimally invasive approaches.
- The locking compression plate/screw construct remains the global standard due to its stability, low complication rates, and strong clinical outcomes.
- Surgeons benefit from understanding biomechanical principles, technique variations, and the limitations of minimally invasive methods in achieving durable fusion.
- Ongoing discussion centers on outcomes across horse types, cartilage removal adequacy, and evolving evidence for alternative approaches.
Disclaimer: The article represents the opinion of individual authors exclusively and not necessarily the opinion of AO or its clinical specialties.
Osteoarthritis of the proximal interphalangeal joint
Osteoarthritis (OA) of the proximal interphalangeal joint (PIPJ) joint results from a variety of conditions including repetitive use trauma, acute disruptive injury, developmental disease, and infection. The resulting lameness is a common cause of impaired performance in affected patients. Therapy aimed at improving biomechanics of the distal limb combined with systemic and local anti-inflammatory therapy can temporarily alleviate lameness and allow many patients to perform at an acceptable level early in the disease. However, osteoarthritis of the PIPJ is particularly progressive, usually limiting the duration of relief. Chronic debilitating lameness results. In rare instances, sufficient periarticular new bone forms which eliminates PIPJ motion and alleviates pain. Spontaneous ankylosis is quite rare in the authors’ experience, with most horses experiencing persistent and progressive lameness that typically becomes incompatible with humane standards of care.
Surgical methods to facilitate joint fusion and eliminate pain
Surgical methods to facilitate joint fusion and eliminate pain associated with end stage OA have been utilized in both human and veterinary surgery for many years. Once the OA affected joint is fused and motion is eliminated, the patient becomes pain-free. Return to functional activities is possible, depending on the joint affected. The basic principles of surgical fusion, i.e. arthrodesis, have been well-described and include removal of cartilage and fibrous tissue that prevents contact of the subchondral bone surfaces, alignment at a functional angle, and maintenance of bone apposition until fusion is complete, preferably with transarticular compression.
Arthrodesis of the osteoarthritic equine PIPJ
Arthrodesis of the osteoarthritic equine PIPJ was first reported in the 1970’s. The technique included dorsal disarticulation, removal of all accessible cartilage, fixation using three transarticular cortex screws placed in lag fashion and cast immobilization for 6-8 weeks postoperatively. Successful outcomes were moderate for horses with hindlimb PIPJ-OA and less favorable for those with forelimb PIPJ-OA. Early postoperative lameness, cast associated morbidity and extended hospital stays were the norm, primarily due to the inability of the transarticular lag screws and cast to provide adequate stability in the immediate postoperative period. In the early 1990’s, the technique was modified to include a dynamic compression (DC) plate. The dynamic compression (DC) plate was applied axially to the dorsal aspect of the PIPJ in conjunction with two, transarticular 5.5mm cortex screws placed in lag fashion. The DC plate/screw construct provided substantial improvement in stability of the construct with significant improvement in post operative comfort allowing early cast removal and markedly shortened hospital stays. In addition, return to function was improved for both fore and hind limb affected horses. With the introduction of the PIP locking compression (LC) plate the late 2000s, further improvements were noted, and the LC plate/screw construct has become the global standard. Numerous studies have detailed the very low incidence of complications when compared to most equine orthopedic procedures where open reduction and internal fixation are indicated. Catastrophic construct failure in the early post-operative period has not been reported and postoperative surgical site infection has been reported to be less than 10%.
The opinions expressed below are in response to proposed alternatives to the standard LC plate/screw PIPJ arthrodesis technique and are based on the authors’ 45+ years of experience in equine orthopedic surgery. They result from having performed well over 100 PIP arthrodesis, initially with the 3 screw technique, followed by the DC plate/screw technique (58 cases reported), and LC plate/screw technique (30 cases reported / and an additional 49 cases at our hospital since that report), with the plated cases having been performed using a standardized technique by two ACVS-certified surgeons.
Minimally/less invasive surgery—collateral ligament sparing techniques
Numerous studies have investigated collateral ligament sparing techniques (LST) and equated them with minimally invasive surgery (MIS). We question if the LST approach is truly much less invasive than the standard arthrodesis approach. The main tenet of MIS is leaving the overlying soft tissue envelope largely intact. Implants are placed through a soft tissue tunnel, and screws are inserted via stab incisions. Reducing exposure and tissue disruption is expected to reduce the incidence of surgical site infection. Access for drilling the articular cartilage and placing the implants in the LST involves incising the skin longitudinally and splitting the overlying extensor tendon verses an inverted-T skin incision and inverted-V extensor tendon dissection. Although no skin or tendon flaps are created in the LST, the skin and extensor tendon flaps when formed appropriately in the standard approach have not created significant issues with healing in our experience. When using the standard approach, the skin incision does not overly the inverted-V extensor tenotomy, with the exception of the very apex of the V. The intact tendon provides a soft tissue barrier between the skin incision and the implants. If complications with the skin incision and dehiscence occur following the standard approach, the implant is protected by the overlying tendon. With the LST approach, the tendon incision is directly beneath the dehisced skin incision which would be likely to increase the risk for implant infection.
Advantage of the LST approach—reduced surgical time
Another purported advantage of the LST approach is reduced surgical time. In most reports this equates to about a 30-minute reduction in surgical time. While shortened anesthesia / surgical times are always desired in equine surgery, the majority of PIP arthrodesis performed using the standard technique are completed within a 3-hour time frame. With anesthetic techniques in use today, minimal differences in anesthesia related complications would be likely in a healthy horse undergoing elective surgery, as is the norm for PIP arthrodesis. Furthermore, the infection rate in equine orthopedic surgery have recently been shown to be unrelated to surgery time. This includes a large series of open reduction and internal fixation procedures in a variety of orthopedic surgeries as well as a large case series focused on PIPJ arthrodesis for OA and middle phalanx fractures. While surgical site infection (SSI) is a major concern in all orthopedic procedures, especially when surgery is performed on the distal limb, the standard approach to the PIP has one of the lowest incidences of infection in equine orthopedic surgery reported. At our hospital, the incidence of post-PIP arthrodesis infections in horses which were treated for reasons other than post-infection OA, is currently approximately 7%. In one recent report, an infection rate of 4% was reported with the standard approach. With the exception of one small clinical series, there is a lack of evidence in a large population of patients to support that the LST approach will significantly lower infection rates below the standard approach.
Maintaining collateral ligamentous support
Maintaining collateral ligamentous support of the pastern joint and increasing resistance to catastrophic failure of the bone implant construct is another stated advantage of the LST. In-vitro testing has demonstrated that bending strength of the LC plate/screw construct is greater in the frontal plane with intact collateral ligaments; however, there is no difference in the sagittal plane. The clinical significance of this finding is debatable. It would be important if the patient was recovered from anesthesia without being placed in a cast and if a highly uncoordinated attempt to stand during recovery loaded the digit in the frontal plate. However, to protect the limb during potential abnormal weight bearing forces during recovery, a distal limb cast is routinely utilized and removed 10-14 days post-op to minimize cast related morbidity. Furthermore, loading of the digit is almost exclusively in the sagittal plane when standing or walking as would be expected during the period of bone healing. The lack of any construct failures at our hospital or in any of the numerous case series in the literature is further evidence that there is no additional risk to transecting the collateral ligaments with the standard PIPJ arthrodesis procedure when a cast is applied prior to recovery from anesthesia.
Arthrodesis
Arthrodesis entails surgical removal of the intraarticular barriers to boney fusion, i.e. cartilage and fibrous tissues. The amount of cartilage removal necessary to achieve adequate boney fusion to eliminate joint motion is unknown, but literature supports removing as much cartilage as possible. Ex-vivo studies on LST have primarily focused on drilling the joint space with a 4.5mm drill bit, in a dorsal trajectory alone or combined with lateral to medial drilling, with or without fluoroscopic guidance. Cartilage removed by joint drilling was typically less than 50%. Importantly, drill tracts were separated by 1cm of articular tissue, effectively preventing contact between the exposed subchondral bone.
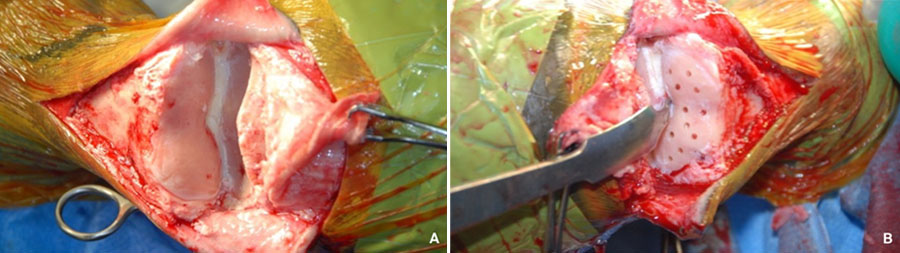
A described LST modification entails incising the dorsal joint capsule and curettage of the dorsal articular cartilage facilitated by joint distraction using elevators. In this ex-vivo report, the percentage of total cartilage removal was similar to other LST reports. Remaining cartilage was primarily in the palmar / plantar aspect of the articulation which would allow more effective apposition of the subchondral bone dorsally. In that same report, when the PIP joint was disarticulated dorsally using the standard technique, removal of 90% of the articular cartilage was achieved. In clinical cases of early to mid-stage OA, we routinely remove well over 90% of the OA cartilage by curettage (Fig. 1).
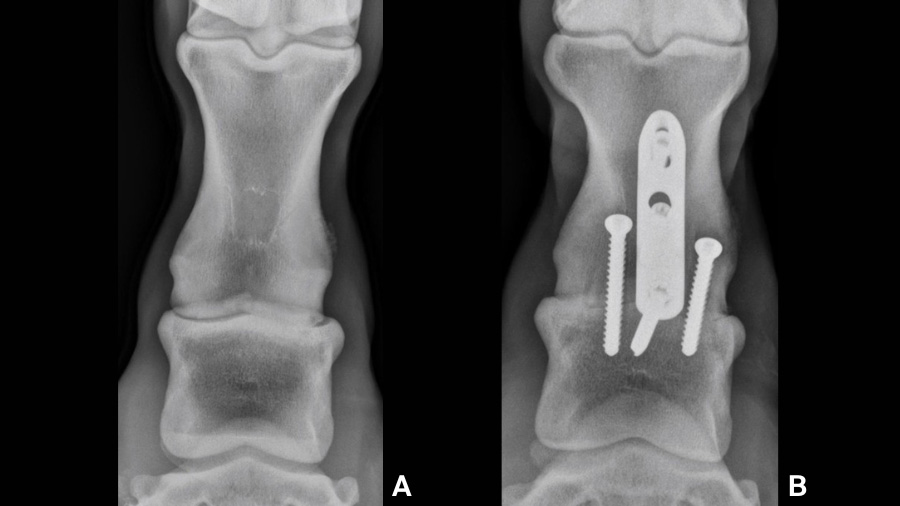
In addition, the standard approach provides adequate exposure for performing osteostixsis of the subchondral bone facilitating access to the healing elements beneath the subchondral plate. When the joint is realigned and implants are placed appropriately, excellent compression between the subchondral bone surfaces throughout the joint is attained. Compressing the subchondral plates together provides friction between the exposed subchondral bone, increasing stability to the bone-implant construct verses relying solely on the implants. Maximal stability is achieved, favoring bone healing and improving patient comfort in the early post-operative period. With the cartilage drilling LST approach, the subchondral plates will be separated by the remaining articular tissues, obviating any contact, let alone compression, between the exposed boney surfaces. The implants will provide construct stability but frictional forces will not contribute. Although it is expected that the remaining articular tissues will eventually degenerate and allow further bone formation, this is not well documented in horses. In one equine study utilizing the LC plate/screw construct combined with a single lateral to medial drill tract augmented with tissue engineering, there was considerable cartilage degeneration over the 4-month period of the study. However, when examined histologically, the tissue filling the drill tract was largely fibrous tissue with only minimal woven bone. Lastly, many patients with PIP-OA experience asymmetric cartilage loss resulting in a valgus or varus deviation at the joint. Removing the remaining articular cartilage allows realignment of the PIP joint, normalizing weight bearing forces through the digit (Fig. 2). This is expected to lessen stress on adjacent structures and contribute to positive outcomes. This is not possible with the cartilage drilling technique.
Advanced osteoarthritis
Patients with very advanced OA, pose a slightly more difficult situation. Periarticular new bone formation combined with soft tissue fibrosis make dissection and dorsal disarticulation more challenging. Although radiographs may suggest that partial fusion will prevent access to the PIP, it has been our experience that it is a rare exception. Although intra-articular access may not be to the degree possible in the less affected joint, we have been successful in exposing and curetting the majority of intra-articular tissues in nearly all patients with advanced OA.
A single case series detailing results of LST and partial cartilage removal by articular drilling (AD) in advanced OA cases have been published. Most patients in that report were not expected to perform athletically, and outcomes were considered successful if the patient’s lameness improved and were considered successful for light riding. In that report two of eleven patients returned to athletic use with the remaining horses improved but still grade 2 or 3 lame at follow-up evaluation. While it is unknown if incomplete arthrodesis was the cause of the unresolved lameness in that report, when compared with the numerous studies following arthrodesis using the standard technique, substantially more patients returned to intended use, including performance beyond light riding. Using the standard PIP arthrodesis technique on a population of primarily western performance horses, we have achieved excellent results, with 85% horses used for athletic purposes and many of the remaining horses used for light riding.
LC plate / screw construct variations
The standard construct for PIP arthrodesis consists of two abaxial, transarticular 5.5mm cortex screws placed in lag fashion with an axially positioned 3-hole PIP-LC plate (Fig. 3).
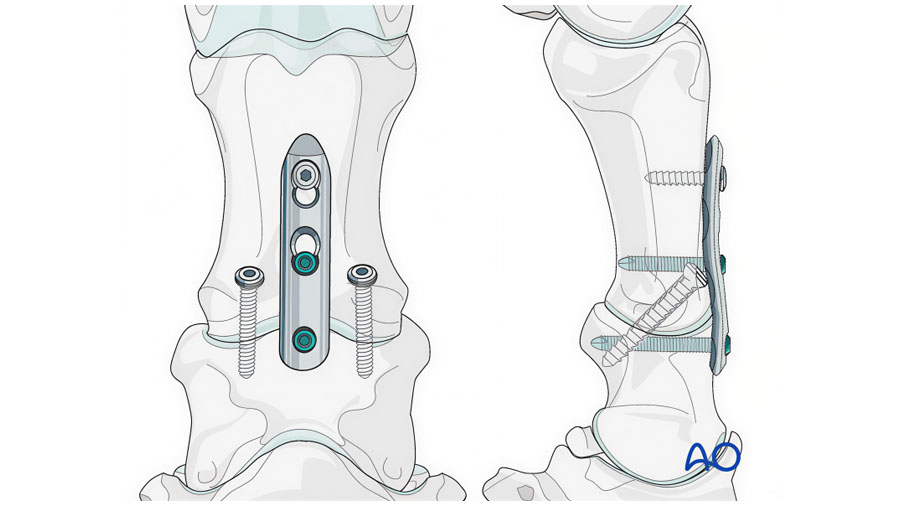
The stacked combi-hole (H1) is positioned just distal the subchondral plate of the proximal aspect of the middle phalanx with the remaining combi-holes overlying the proximal phalanx, the middle combi-hole (H2) lies adjacent to the joint in the distal aspect of the proximal phalanx, and the most proximal combi-hole (H3) is near the diaphysis of the proximal phalanx. Palmar/plantar transartricular compression is achieved with the transarticular lag screws. Dorsal compression is accomplished by initial placement of a 5.0mm locking screw in H1 followed by the unicortical cortex screw in H3 placed in the load position. When the cortex screw in H3 is fully tightened, dorsal compression is achieved. Angle stable fixation is accomplished by placing a 5.0mm locking screw in H2 of the plate.
Major variations in the above technique include placing the compression generating cortex screw in H2 and using a bicortical locking screw in H3, using a bicortical screw in H3 instead of a unicortical screw, and placing additional transarticular screws abaxially. All of these provide an acceptable construct and meet the criteria for arthrodesis when applied using the standard approach with removal of all accessible articular cartilage. Whether any of the above variations are clinically superior or improve patient outcomes is debatable and will require further investigations documenting results in a large number of patients. The rationale for the construct performed at our hospital is discussed below.
Biomechanical advantages of locking plate technology
Biomechanical studies of locking plate technology have established that locking screws are most advantageous when placed immediately adjacent to the area of instability. The biomechanical advantage of locking technology diminishes with increased distance of the locking screws from the area of instability. With regards to generating compression, there is no difference in the amount of compression generated whether the cortex screw is placed in H2 or H3, as the max amount of displacement with a single screw in the load position will be 1mm when placed in either position. A potential advantage of placing a cortex screw in the H2 position is greater compression of the plate to the underlying bone. We ensure plate-bone compression by placement of the push-pull device in H2 during plate positioning. Although the degree of plate to bone compression is likely superior with the cortex screw in H2, we believe that having the plate on the bone, achieved with the push-pull device, and using a locking screw adjacent to the joint provides a better overall biomechanical outcome by utilizing the full potential of the locking technology. However, there are no biomechanical studies available to either support or refute the advantages / disadvantages of these constructs. Both are used with success clinically, with ample evidence published which supports the standard construct. Published evidence of this variation to with which to compare outcomes is clouded by inconsistencies in the constructs reported.
Rationale for use of a unicortical cortex screw
The rationale for use of a unicortical cortex screw in H3 has been questioned. In our initial biomechanical study using a bicortical screw in that location, the majority of failures in DC plate/screw construct occurred by transverse fracture at the proximal aspect of the plate propagating through the screw hole in the palmar cortex of the proximal phalanx, clearly demonstrating the stress concentrating effect in the region. Other ex vivo studies have demonstrated different failure modes lessening the concern for stress concentration at the proximal aspect of the plate. The lack of clinical evidence demonstrating construct failure at any location, further resolves any concern for stress concentration resulting in catastrophic failure of the plate/screw construct regardless of variations in screw type or placement. This includes both perioperative failures as well as during performance once healing is complete.
We continue to employ a unicortical screw in the H3 position as we have not encountered any negative consequences. One report has questioned the ability of a unicortical screw to effectively create compression when placed in the load position and argued that a bicortical screw is necessary for that purpose, otherwise toggling of the screw would occur mitigating the compressive effect of the screw. Although this could occur in bone with a very thin cortex or poor quality osteopenic bone, it would be readily apparent to the surgeon when the screw is tightened. The evidence for this occurring in PIP arthrodesis in a typical candidate for the procedure is debatable. The dorsal cortex of the mid-diaphysis of the proximal phalanx in the horse is of robust thickness and density and provides adequate working length for the screw to function as intended. In our experience, toggling of the screw and failure to provide compression has occurred in only one patient out of the multitude of patients treated in our hospital. This includes numerous patients less than a year old as well over 20 years old, many of which had chronic severe lameness and might be expected to have lower quality bone. Furthermore, when this argument was initially proposed, evaluation of the angle of unicortical screws before and after tightening among our clinical cases failed to demonstrate any evidence of toggling (Fig. 4).
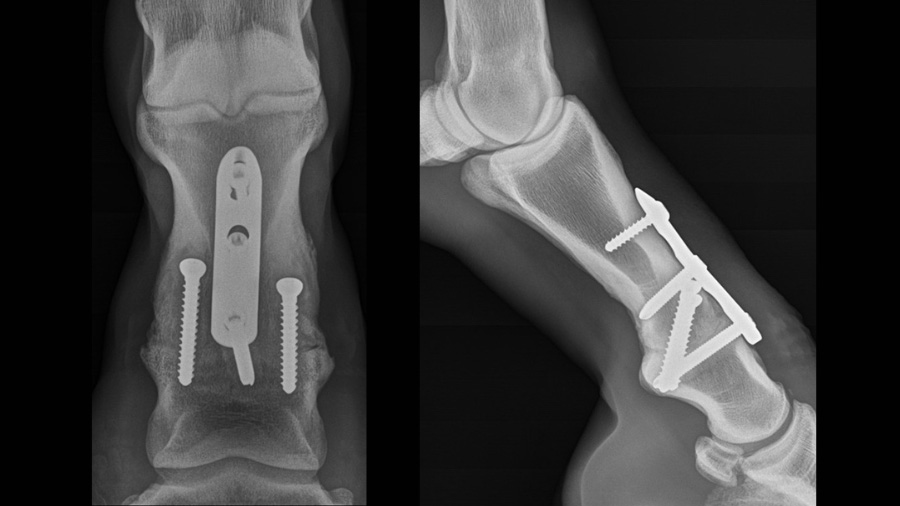
However, in the rare instance it might occur, it would be readily apparent to the surgeon and easily remedied by replacing it with a bicortical screw.
Additional rational for continued use of a unicortical screw relates to the long-term function of the patient. It is well accepted that screws transfixing the dorsal and palmar cortices in the metacarpal diaphysis can cause pain once the patient returns to performance activities. Although hypothetical, it is possible that a bicortical screw in the H3 location, which transfixes the dorsal and palmar/plantar cortices in the mid-diaphysis of the proximal phalanx, could cause pain and affect performance. Whether avoiding this by use of a unicortical screw has contributed to the high rate of success in our patient population remains to be elucidated.
Transarticular screws
The final construct variation is additional transarticular screws. The majority of our clinical patients are Quarter Horses who typically have a relatively small bone stature when compared to Thoroughbred and Warmblood breeds. In small stature patients, the amount of bone available abaxial to the plate is limited due to the size (width) of the proximal and middle phalanges. This limits the number of screws which can be placed comfortably on each side of the plate. In large stature horses with wider phalanges, there is often ample room for additional transarticular screws on both sides of the plate. It stands to reason, that when additional transarticular screws can be accommodated, they would add to the strength of the fixation, especially when the joint is dorsiflexed at high loads. However, it is not clear if additional compression can be generated across the articulation by adding more screws. A major advantage would be in cases where there is partial or complete disruption of the palmar/plantar soft tissue support structure resulting in subluxation or luxation in the palmar/plantar direction. In small stature horses, these forces are neutralized by double plate fixation due to the inability to add additional transarticular screws. However, in large stature horses, additional transarticular screws may be a suitable alternative to double plate fixation. There is ex-vivo work that shows biomechanical improvement over the standard construct in pasterns; however, it is unclear if the difference would be significant with intact palmar/plantar soft tissue support. Whether additional screws provide a clinical benefit in a routine arthrodesis with intact palmar/plantar support remains to be determined. What is clear, is that outcomes have been very good with the standard construct in a large number of patients.
Interpretation of published results—biomechanical and clinical
Ex-vivo studies documenting the biomechanical behavior of differing plate/screw constructs are useful to gain a better understanding of the ability of the implants to neutralize forces acting at the arthrodesis. Fixation strength is important relative to preventing catastrophic failure. Stability is important relative to boney healing across the joint as well as patient comfort. Fatigue life predicts the ability of the construct to maintain its strength and stability during the healing period before the boney structures are restored to weight bearing capacity. All of these parameters have been the subject of investigations published to date. The challenge in interpretation is the lack of continuity in testing methodologies. With rare exception, the constructs fail to represent the clinical situation to the extent possible. Most notably, some studies have removed the periarticular soft tissue support, which plays a major role resisting plantar/palmar displacement.
Furthermore, the majority of constructs evaluated ex-vivo have not included cartilage removal. Intact cartilage disallows any degree of compression between the subchondral bone plates of the proximal and middle phalanges. Interfragmentary friction generated by compressive fixation plays a critical role in stability. It is unclear if any of the proposed variations in construct configuration increase the mechanical attributes of a PIPJ arthrodesis to a significant degree over a standard construct in the clinical scenario with intact palmar/plantar soft tissues and compressive fixation following complete cartilage removal. Other challenges include variations in mounting the specimens in the testing apparatus and applying load to the constructs. It is well accepted with ex vivo testing that it’s not possible to accurately reproduce the in vivo loads on the constructs. This results in major difficulty interpreting the results of ex-vivo studies to the clinical setting.
Retrospective studies
Few, if any, orthopedic procedures in equine surgery have been the subject of more clinical retrospective studies than arthrodesis of the PIP joint. The common occurrence of OA and injury to the PIP joint has resulted in most of these reports including reasonable numbers of patients from which to draw conclusions. However, many reports are the compilation of patients over an extended period of time with the arthrodesis performed by a number of different surgeons, all of which perform the procedure according to their individual preferences, adding variability to the results. While most studies report positive outcomes and high client satisfaction rates, the definitions for outcomes are not uniform. Further variability exists in patient populations, conditions treated, and follow up of sufficient duration into the post arthrodesis career as a performance horse to be meaningful. This has become of particular interest when comparing outcomes for horses involved in English performance compared to Western performance.
English performance following PIP arthrodesis in the forelimb
There is anecdotal data suggesting outcomes are significantly inferior for the patients returning to English performance following PIP arthrodesis in the forelimb. As noted previously, most of our clinical experience has been in breeds considered to have small bone stature (although their bone structure is relatively small, many are 500-550 kg in body weight) where we have experienced only a small difference in positive outcomes between fore and hind limbs. The disparity in outcomes between these patient populations, if true, may be due to an inability of the standard technique to provide the necessary mechanical environment to support the fusion in patients of greater size and body weight, or some other biomechanical issue. If it’s the former, perhaps a more robust fixation is needed. Determining if additional transarticular screws will improve this shortcoming will require documentation of the outcomes in a sizable number of horses within that population. Another consideration which has likely influenced the positive outcomes in our patient population is the type of activity the horse is expected to perform. Most Western performance horses are expected to perform at speed, with the ability to make abrupt changes in direction, as well as stopping quickly. The surfaces they are working on are usually soft with a reasonable degree of cushion. It is feasible that a degree of lameness can be tolerated in these patients without affecting their post-operative performance. It may be that in English performance horses, differing footing and mild asymmetry in gaits cannot be tolerated and therefore these patients may be held to a higher standard when assessing positive outcomes.
Our desire is to return our patients to their former level of performance
Ultimately, our desire is to return our patients to their former level of performance and have a client who is satisfied with the monetary investment in the procedure. Adhering to the AO principles of open reduction and internal fixation, including the application of dynamic compression with the plate/screw construct, in conjunction with principles of arthrodesis, including complete cartilage removal, has enabled many horses with conditions of the proximal interphalangeal joint to return their intended use.
About the authors:

Dr Jeffrey Watkins, DVM, MS, DACVS is a board-certified surgeon with over 40 years of experience in equine orthopedic surgery. He earned his DVM from Kansas State University in 1980, complete an internship and surgical residency at Texas A&M, earning a Master of Science degree in 1984 and became board certified in surgery in 1986. Dr Watkins became a member in the Department of Large Animal Clinical Sciences in 1983 after completion of his residency. He has served as Chief of Surgery and Section Leader of the Equine Orthopedic Service. He was promoted to professor in 1999. He was recently appointed to the position of Senior Professor. In addition, he holds the Linda and Dennis Clark ’68 endowed chair in equine studies.
Dr Watkins has a long history of involvement with the AO, serving as faculty for both AO VET NA and AO VET International. As a member, and later as chairperson of the Veterinary Expert Group and Large Animal Working Group, he contributed to the development of a number of innovations in the equine portfolio, including the locking PIP arthrodesis plate. He has served AO as chairperson of AO VET NA and is currently in his second term as chairperson of AO VET International.

Dr Kati Glass is a Clinical Associate Professor and Chief of Surgery at the Texas A&M College of Veterinary Medicine & Biomedical Sciences' Veterinary Medical Teaching Hospital. She graduated summa cum laude from Texas A&M College of Veterinary Medicine & Biomedical Sciences with her DVM in 2012. She completed an internship at Equine Medical Center of Ocala prior to a surgery residency at Texas A&M in 2016. Kati became a Diplomate of the College of Veterinary Surgeons (Large Animal) in 2017 and has been AO Faculty since 2018. She is a member of the Education Committee for AO VET NA and served on the Large Animal Working group of the Veterinary Expert Group. Her primary clinical interests are in orthopedic trauma, sports medicine, and advanced imaging.
You might also be interested in...

Principles in Equine Fracture Management
This course covers the first aid, diagnosis, and case selection for simple fractures, osteoarthritis of the pastern joint, and simple angular limb deformities.

AO VET Webinar—Equine
This webinar presents computer assisted surgery, and discusses fracture diagnosis and planning.

AO Surgery Reference: Horse
A resource for the management of fractures, based on current clinical principles, practices and available evidence.