Decision-Making in Feline Orthopedics: One Size Does Not Fit All!
BY KAREN PERRY

Our clinical experience, in addition to the expanding peer-reviewed literature, suggest differing approaches may be indicated when treating traumatic injuries in cats compared to those adopted in dogs. Of course, anatomical differences must be considered, and treatment adapted to feline specifics, but going further than that, every fracture is unique and different approaches may be warranted in certain situations. With developing inventory, numerous options are now available for feline fracture repair and in order to achieve optimal results in our feline patients, detailed preoperative planning taking mechanical factors, anatomical site factors, patient factors and biological factors into account is essential. While two fractures may appear radiographically very similar, varying factors can cause us to choose different approaches to fixation. In this post, we are going to look at some cases, that despite their very similar radiographic appearances, had varying mechanical, patient, or biological factors. The impact of these factors on the surgical approach taken will be discussed emphasizing the importance of keeping your options open and developing a tailored treatment plan for each individual.
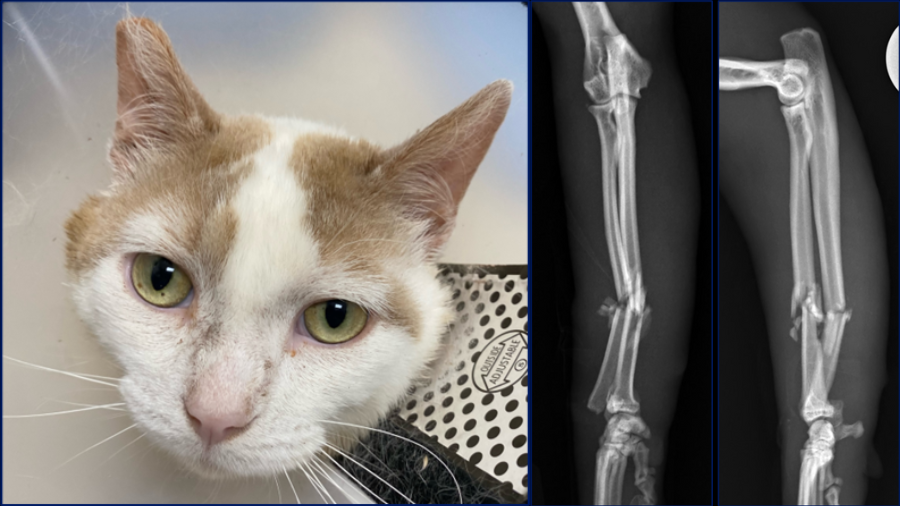
Here are three radius and ulna injuries in three young cats. Feline antebrachial fractures are relatively infrequent comprising only 3-8% of all fractures in cats. This is in contrast to dogs where antebrachial fractures are the third most common limb fracture with a prevalence of 18%. A recent study1 used microcomputed tomography to compare the trabecular and cortical bone microarchitecture of the radius and ulna in cats and small dogs and showed that cats have higher bone volume fraction, thicker trabeculae, increased anisotropy and significantly higher diaphyseal cortical density which may contribute to the lower fracture risk in this area in cats. Fracture distribution may also be different in cats when compared to dogs, in that most fractures are mid-diaphyseal, followed by proximal and then distal diaphyseal. This contrasts to what is seen in dogs where radius and ulna fractures are predominantly located in the distal and middle thirds with very few proximal fractures.
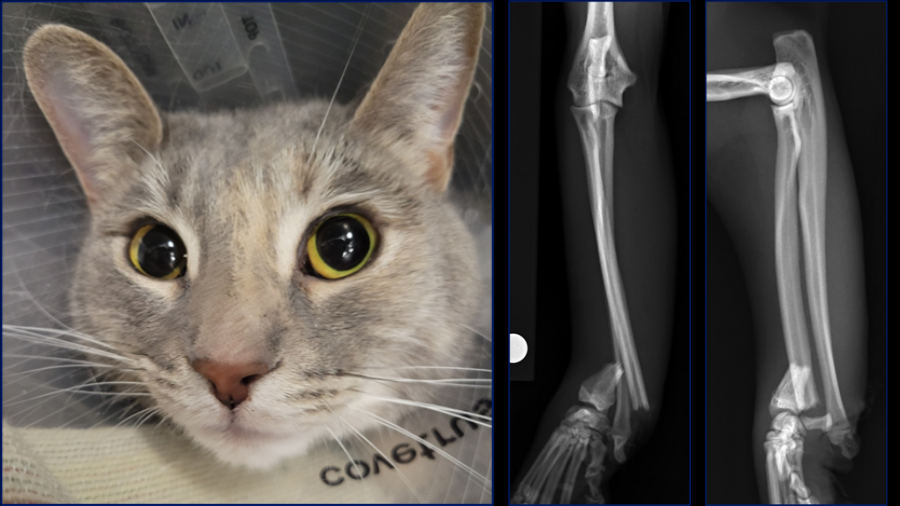
Case 1: Bundle, one-year-old female spayed Siamese cat with an acute onset of non-weight bearing left forelimb lameness
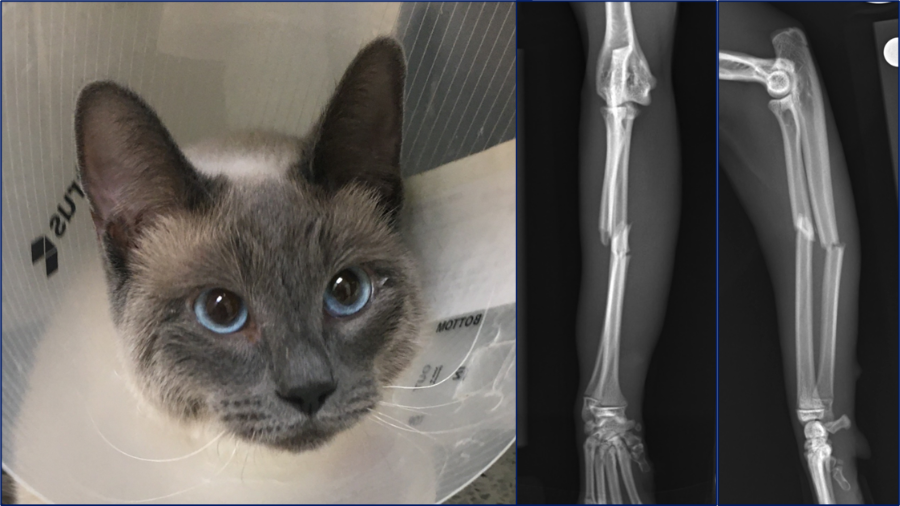
I would like to start by discussing case considerations for the first case which is Bundle, a one-year-old female spayed Siamese cat. She presented with an acute onset of non-weight bearing left forelimb lameness after playing with her sibling. On orthopedic examination she had instability upon palpation of the left antebrachium, with associated swelling and crepitus.
Generally, feline radius-ulna fractures are associated with a high complication rate; similar to that seen in toy and small breed dogs. This is proposed to be because of the complex paired bone system and the relative mobility of these bones in the cat. It is postulated that the increased range of motion of the feline antebrachium may increase the relative movement between the radius and ulna fracture sites, thus increasing interfragmentary strain and the potential for major complications such as non-union.
In one study,2 23% of cats suffered major complications requiring revision surgery following their first repair. This revision surgery rate is similar to, or worse than, revision surgery rates for toy breed dogs where rates of 7-18% have been reported. In the feline literature, mid-diaphyseal and proximal diaphyseal fractures are more likely to require revision surgery; and as Bundle’s fractures are mid-diaphyseal, they fall into this higher risk category.

There are several treatment options that may be considered here, all with associated advantages and disadvantages. External coaptation might be considered in medium-to-large breed dogs with transverse radius and ulna fractures but generally is only considered for minimally displaced fractures or in cases where finances preclude surgical stabilization. Additionally, cats do not tolerate external coaptation well and it can be high maintenance for owners, particularly regarding keeping it clean during litter tray use, so I would not consider this a good option for this case.
External skeletal fixation (ESF) could be used here using either a type 1 or type 1b frame. Advantages of this approach would be the potential for a biologic approach and the fact that all the implants would be removed. One disadvantage of ESF for this fracture, however, is that as this fracture is mid-diaphyseal, the ESF would have to be applied proximally. ESF application here is more complex due to the increased soft tissue coverage and the proximity of the elbow joint. Additionally, the oval shape (flattening in the mediolateral plane) and mild curvature of the radial shaft render ESF pin placement challenging in the mediolateral plane. Finally, the feline radius has a pronounced tapering distal to the radial head which may predispose it to fracture at this point, particularly following ESF pin removal and a higher complication rate has also been reported following use of ESF when compared to radial plating for radius-ulna fractures in cats.
When plating is selected, while cranial plating is far more commonly performed, medial plating has also been reported in four cats.3 Advantages of medial plating include additional screw purchase because of thicker mediolateral bone diameter, closer spacing of the screw holes as a smaller plate can be used because it is edge-loaded and avoidance of the extensor tendons in the area of the distal radius. These advantages make medial plating particularly attractive for use in distal fractures with a paucity of bone stock. Inadvertent purchase of the ulna with screws is also less likely with medial plating so this may be useful in young cats where discrepant growth between the radius and ulna remains a concern, or in cases where we particularly want to avoid a synostosis to preserve pronation and supination. In the study including four cats, 2.0mm DCP plates were used medially on the feline radius. All cats had good long-term outcomes, but two cats had implants removed at 5 and 7 months post-operatively. The authors state that they routinely removed implants at this time, but it is not explained why in the paper. Therefore, it is difficult to know if the rate of implant removal would be different between medial and cranial plating techniques.
It has been reported that the complication rates associated with feline radius-ulna fractures are substantially higher when one bone is stabilized compared to when both are stabilized.2 One study showed that when both bones were stabilized, 12.5% required revision, in comparison to 31% of cases when only one bone was stabilized. While a more recent study failed to demonstrate the same results,4 rendering further research in this area warranted, the fractures in that particular study were predominantly distal diaphyseal, and as these are associated with superior outcomes in cats, it remains unknown whether these results can reliably be applied to the higher risk mid- and proximal-diaphsyeal fractures. Dual bone fixation has been shown to increase construct stiffness and strength and may reduce the risk for synostosis formation hereby preserving pronation and supination which are considered critical for normal function in cats.
As mentioned previously, cats have a far greater ability to pronate and supinate the antebrachium and forepaw than dogs. Due to this movement of the paired bones, fixation of the radius or ulna alone is less likely to result in stable fixation of the adjacent bone. As dual bone fixation has historically been shown to have lower complication rates, several authors recommend that dual bone fixation be considered for feline radius-ulna fractures and certainly this remains my technique of choice, using either an intramedullary (IM) pin in the ulna, or an additional plate laterally on the ulna in conjunction with radial plating. As such, these options were also considered for Bundle.
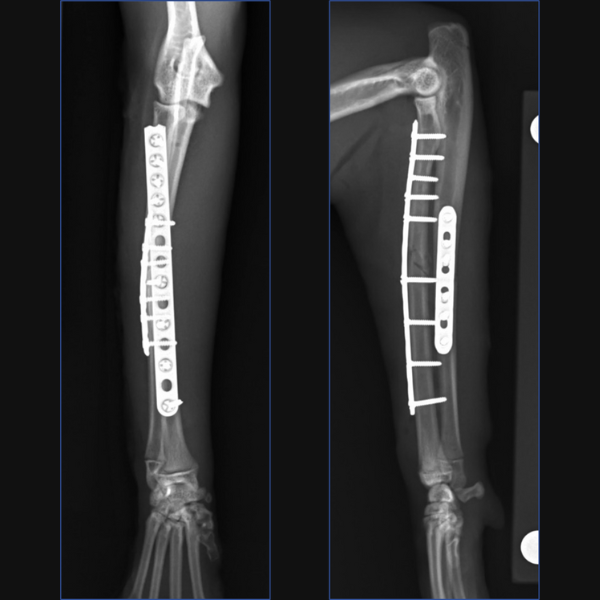
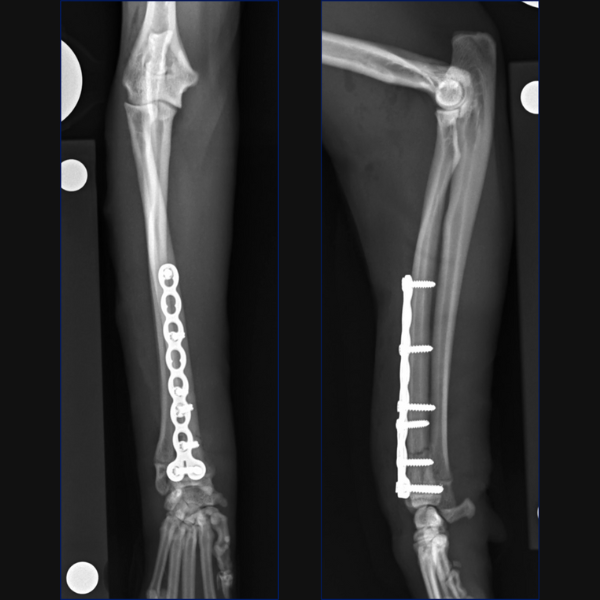
For Bundle we performed open reduction and internal fixation using a 14-hole 1.5/2.0 Veterinary Cuttable Plate (VCP) on the radius and a 6-hole 1.5mm Locking Compression Plate (LCP) on the ulna. This was all performed through single craniolateral approach. I think we have addressed one reason why we chose dual bone fixation in this case, due to the lower complication rate that could be anticipated with that. Another reason is that in people at least, insufficient stabilization has been associated with an increased risk of synostosis formation so rigid, dual-bone fixation was desired here to limit that. But why choose a lateral plate on the ulna rather than an IM pin?
Mechanics is one consideration here: Preston and others compared the biomechanical properties of two dual bone fixation (DBF) constructs to isolated radial locking compression plating in an ex vivo feline antebrachial fracture gap model back in 2016.5 All groups had a cranial 2.0mm LCP placed on the radius. One dual bone fixation group received a 1.2mm ulnar IM pin and one received a 2.0mm LCP on the ulna. Not surprisingly, DBF constructs were significantly stiffer than the radial LCP alone in axial compression and caudocranial bending. There were no differences between LCP with pin and dual plate constructs in axial compression, caudocranial bending or mediolateral bending. However, failure load was significantly greater for dual plate constructs than for the plate-pin construct, with failure loads for the pin-plate construct not being different to the plate alone. Now, there are certainly some limitations to that study; one notable one is that the antebrachii were potted specifically to retain the relationship between the bones while uniformly loading them during testing. This meant that the radius and ulna could not move independently and therefore, this likely does not replicate in vivo conditions. Additionally, torsional stability was not assessed in this study at all. However, given our desire for rigid fixation in a very active cat with a presumed high risk of synostosis, the dual plating option was elected. I am more likely to choose an IM pin as the method of stabilization for the ulnar fracture in cases where the fracture is more distal, and the risk of synostosis maybe lower, and where I can easily place the IM pin normograde from distally in the shorter distal segment, therefore avoiding additional soft tissue dissection at the fracture site to facilitate retrograde placement, or the creation of an additional approach proximally and potential irritation of the triceps which is associated with normograde insertion from proximally. While there is limited information on this technique in cats specifically, the use of an IM pin in the ulna to facilitate minimally invasive plate placement on the radius has been reported in dogs,6 and while the technique was uniformly successful, pin removal was recommended once fracture healing had been achieved, so dual-plate placement may be preferable in terms of avoiding the need for this.
You could debate the choice of a single approach for fixation here based on some literature in the human field. I have generally preferred a single approach with the suture line not lying directly over either of my implants but that is simple personal preference. While it is based on a very specific posterior approach to the radius and ulna called the Boyd approach, and may not be transferrable to our feline patients, there is some evidence in humans with radius-ulna fractures that placement of dual bone fixation through a single approach is associated with a higher risk of synostosis formation than placement of implants through two separate approaches. Postulated reasons include extensive soft-tissue exposure, increased risk of development of radioulnar hematoma or interosseous damage and potential malpositioning of one of the implants due to suboptimal exposure of both bones. Further research is required to determine whether single or dual approaches may be associated with different complication rates in cats, but certainly, you could argue that the radial plate is positioned slightly too laterally at the proximal extent here and that a single approach may have contributed to that.
In terms of critiquing my postoperative radiographs here from Figure 3, in addition to the radial plate being slightly too lateral at the proximal extent, the first screw distal to the fracture is close to caudodistal extent of the short oblique fracture line. This may have rendered this screw monocortical and additionally, may have caused some fragmentation of the fracture line at this point, so not ideal, but we do have an additional three bicortical screws distally on the radius in addition to three screws in the ulna so I did not consider that this warranted any immediate revision surgery.
For Bundle, we prescribed courses of robenacoxib and gabapentin, advised dust-free litter, e-collar use and strict activity restriction for 6-8 weeks and set up recheck appointments at 3 and 6 weeks postoperatively.
Radiographs at 3 weeks postoperatively showed maintained alignment and apposition, appropriate levels of activity and no evidence of implant-associated complications.

Case 2: Charley, 3-year-old male intact domestic shorthair with a non-weight-bearing left forelimb lameness
So, what is different for case 2? Charley was a 3-year-old, male intact domestic shorthair who disappeared and returned two weeks later with a non-weight-bearing left forelimb lameness. There was palpable instability at the level of the mid-to-distal antebrachium and moderate-to-severe firm soft tissue swelling surrounding this region. There was also instability of the left carpus under valgus stress. So – similar to with Bundle, we have the inherently high complication rate associated with radius-ulna fractures in cats, particularly in the mid-diaphyseal region. The revision surgery rate has been reported to be even higher for cats with comminuted fractures, so, Charley is at a higher risk than our first case in that respect. This is also reported in people, where comminuted fractures are associated with higher complication rates and synostosis rates. Similarly to our first case, the radius and ulna fractures are also at the same level and so associated with a higher risk of synostosis. Additionally, there is an ulnar styloid fracture which is causing carpal instability and therefore this needs to be addressed.
This fracture is also presumed to be chronic due to the cat being missing for two weeks, the very firm swelling that was palpable around the fracture site and the slight rounding of the fracture ends which can be seen radiographically. While there is no evidence specific to radius-ulna fractures in cats regarding this, in humans, radius-ulna fractures that undergo delayed treatment are considered at a higher risk of complications, including synostosis formation. Studies have shown that the fracture hematoma favors healing and that removal of the fracture hematoma after several days is more detrimental to healing than when the hematoma is removed earlier.7 Additionally, studies published back in 20128 and 20139 showed that in dogs, radius and ulna fractures treated via minimally invasive plate osteosynthesis (MIPO) had unchanged alignment and gap width when compared to fractures treated via open reduction and internal fixation (ORIF), but that those treated via MIPO did heal more rapidly. Due to this, we did consider that there could be some advantages to minimally invasive osteosynthesis (MIO) in this case. However, cases treated minimally invasively do heal via more proliferative callus formation, so, a downside of an MIO approach could have been a higher risk of synostosis formation? Additionally, reduction was considered likely to be more difficult in this case due to the chronicity so that would complicate an MIO approach.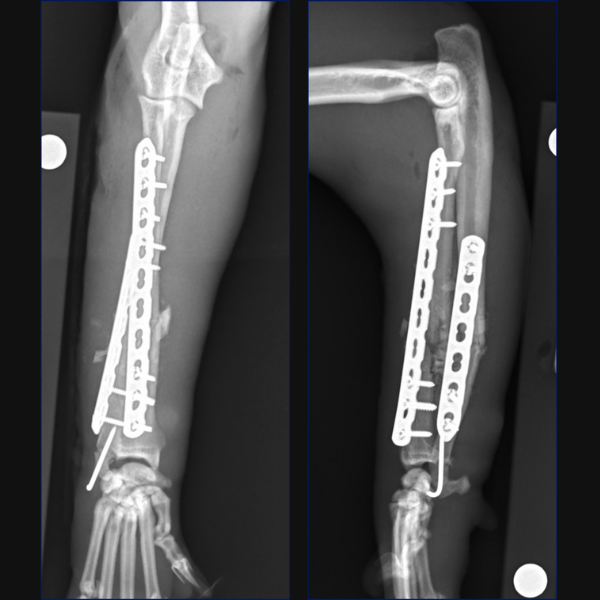

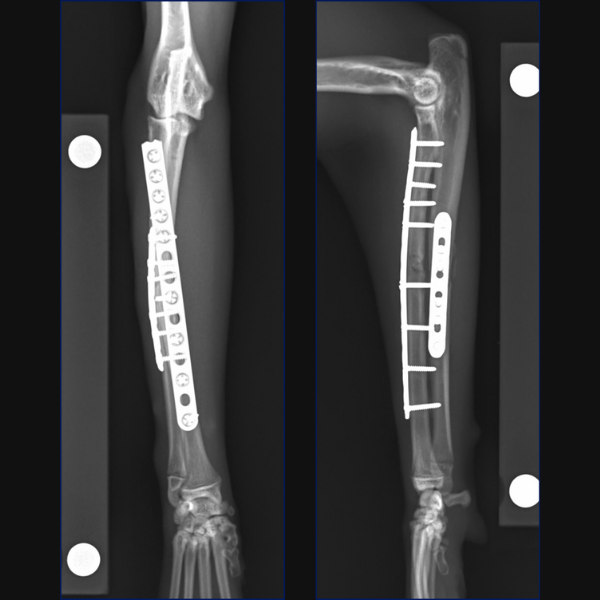
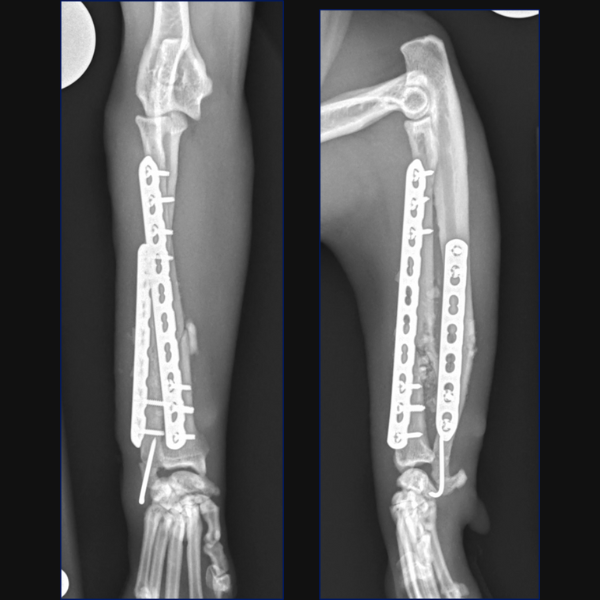
After weighing the advantages and disadvantages, we elected to use a minimally invasive approach here. As anatomic reduction was not going to be possible due to the comminution, we elected to preserve the fracture hematoma and prioritize rapid healing and accept the potentially higher risk of synostosis formation.
Separate minimally invasive approaches were made for the radial and ulnar fractures to facilitate placement of a 10-hole 1.5/2.0 LCP cranially on the radius with 3 screws proximally and 3 distally. A 7-hole 1.5/2.0 LCP was then placed laterally on the ulna through proximal and distal stab incisions. Lastly, the ulnar styloid fracture was stabilized minimally invasively through a stab incision using a 1.2mm K-wire.
The postoperative care advised was identical to that for the first case, Bundle.
Case 3: Missy, 18-month-old domestic shorthair with an open wound at the level of the carpus
So, what is different for case 3? Missy, an 18-month-old domestic shorthair, was found in the bathroom with an open wound at the level of the carpus. As she was bright and alert the owner elected to wait until the following day to have her evaluated. At that point, an open fracture was diagnosed and she was referred for stabilization. At the time that she presented following referral, 36 hours post event, no medications had been given.
So, similar to our first two cases we have the inherently high complication rate associated with radius-ulna fractures in cats, but this one is distal, and not comminuted and so maybe at a lower risk. However, the fracture being distal does also mean that we have less bone stock available so we will likely have to consider T- or L-shaped plates to gain sufficient screw purchase in the distal segment, and locking implants may be of benefit.
However, we also have an ulnocarpal luxation here, which is a very unusual injury in cats. In people this is termed a Galeazzi fracture-dislocation and it is commonly associated with a high velocity direct impact with forceful forearm pronation. In humans, uniform surgical management comprising open reduction and internal fixation of the radial shaft fracture is well described in the literature and the importance of assessing for disruption of the distal radial-ulnar joint is emphasized with damage to the fibrocartilage and interosseous membrane frequently being reported to be under-recognized. Where distal radioulnar joint instability is noted after radial fracture repair, in humans this is managed with supplemental wire transfixion of the distal radioulnar joint or triangular fibrocartilage complex repair. Unrecognized instability can lead to persistent subluxation, which can restrict forearm pronation and carpal extension as well as causing pain, potentially necessitating distal radioulnar joint resection arthroplasty and extensor carpi ulnaris tendon tenodesis. A previous study in humans demonstrated that radial fractures that are more distal are more likely to require stabilization of distal radioulnar joint instability than fractures that are more proximal.10 Given how distal this radial fracture is, we had to consider that stabilization of this joint may be necessary, although there is really no information in the literature about these injuries in cats so this is purely based upon extrapolation from the human literature.
Additionally, this fracture was open, and had not received any antibiotic therapy 36 hours post-incident. As such, we had to consider the increased risk for complications associated with that, notably delayed or non-union, infection and a requirement for subsequent implant removal, which based on a recent study that we conducted at MSU, is approximately 20%.11
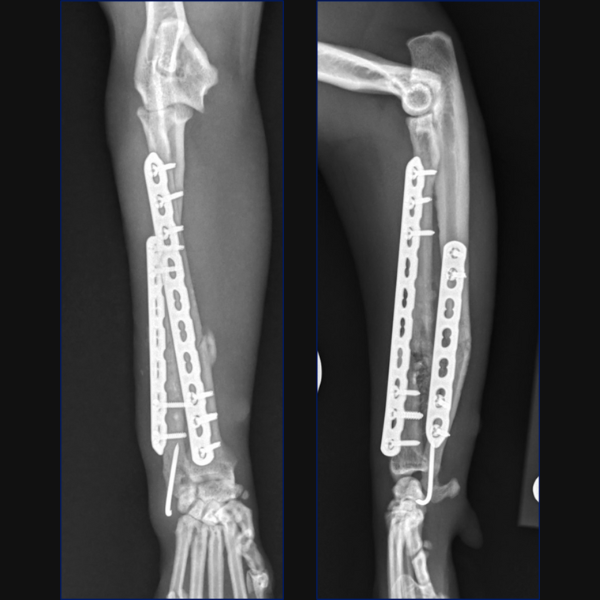
For this case, as anatomic reduction was possible, an open approach was elected with stabilization of the radius being achieved through a craniolateral approach and use of a 1.5/2.0 notched T-plate. 3 locking screws were placed distal to the fracture site with 2 locking and 2 non-locking screws being used proximally. Compression was attempted, but you can see that a small gap remains on the transcortex, so I could have pre-stressed my plate a little better.
Reduction of the radial fracture completely reduced the ulnocarpal luxation. We assessed for instability intraoperatively using the same technique which is reported in people which involves stabilizing the radiocarpal joint with one hand and then trying to move the ulna independently in a dorsal and palmar direction. Based on our assessment, no instability was palpable and as such, no distal radioulnar fixation was considered necessary.
The postoperative care advised here was very similar to that for cases one and two, excepting that a two-week course of potentiated-amoxicillin was also advised. Unfortunately, Missy’s owner was unwilling to return for the scheduled follow-up as she stated Missy was doing very well, so unfortunately, we only have remote follow-up based on owner assessment. The owner states that Missy’s lameness has resolved, and she has not suffered any clinically evident infection or implant-failure. As the fracture was stabilized 16 months ago now, we consider clinically-relevant complications to be unlikely.
We did complete the Feline Musculoskeletal Pain Screening Checklist (Feline MiPSC) with the owner over the phone. This was recently developed in an effort to increase awareness of osteoarthritis in cats, to provide a quick, easy and practical tool for screening of cats for osteoarthritis-associated pain, to be used as a foundation for discussion of feline osteoarthritis with owners and to establish the need for further veterinary investigation. The Feline MiPSC is comprised of 6 items asking if a specific activity can be performed normally or not.
- Does your cat jump up normally?
- Does your cat jump down normally?
- Does your cat climb up stairs or steps normally?
- Does your cat climb down stairs or steps normally?
- Does your cat run normally?
- Does your cat chase moving objects (toys, prey, etc.)?
If any of the items is scored as a “no” (i.e. the activity is not normal), this should prompt further evaluation with a more detailed screening such as a review of a video taken in the home environment or in-clinic observation and orthopedic evaluation. For Missy, the owner answered all questions as a “yes” so, as far as we can tell based on remote assessment she is doing well but we were really disappointed not to follow-up this particular case in more detail. Specifically we would have been interested to evaluate for any degeneration at the level of the distal radioulnar or ulnocarpal joints so that we could assess whether our decision not to stabilize the distal radioulnar joint was appropriate.
About the author:

After four years at the RVC Dr. Perry moved to Michigan State University where she is currently a Tenured Associate Professor in Small Animal Orthopedics and Section Head of Small Animal Surgery. In 2022, Dr. Perry was also named the Pat Carrigan Professor of Feline Medicine. Dr. Perry’s passion for veterinary education led her to pursue further qualifications in this ever-expanding field. In 2019, whilst at MSU, Dr. Perry completed her Masters of Science in Veterinary Education, the thesis of which focused on the importance of feedback during veterinary residency programs. Due to her knowledge in education, Dr. Perry was elected to serve on the AOVET NA education committee.
Dr. Perry has published widely in the veterinary literature with her main research interests being feline orthopedics, traumatology and the correction of limb deformities associated with patellar luxation. Dr. Perry, an International AO Faculty, created the first AO Master Course in Feline Orthopedics and has presented her work throughout the world including in Colombia, Brazil, Mexico, Russia, Spain, Poland and the UK.
References
1. Planner F, Feichtner F, Meyer-Lindenberg A. The cat as a small dog? – Comparison of trabecular and cortical bone microarchitecture of radius and ulna in cats and small dogs using microcomputed tomography. Vet Med and Sci 2021; 7: 2113-2119
2. Wallace AM, De La Puerta B, Trayhorn D, Moores AP, Langley-Hobbs SJ. Feline combined diaphyseal radial and ulnar fractures: A retrospective study of 28 cases. Vet Comp Orthop Traumatol 2009; 22: 38-46
3. Sardinas JC, Montavon PM. Use of a medial bone plate for repair of radius and ulna fractures in dogs and cats: A report of 22 cases. Vet Surg 1997; 26: 108-113
4. Makar JG, Lai JYK, Simcock JO, Jerram RM, Lai A, Levien AS, Hoon QJ, Hall EJS, Basa RM. Feline radial and ulnar diaphyseal fractures: a retrospective study of 49 cases comparing single bone fixation and dual bone fixation. J Fel Med Surg 2024; 26
5. Preston TJ, Glyde M, Hosgood G, Day RE. Dual bone fixation: A biomechanical comparison of 3 implant constructs in a mid-diaphyseal fracture model of the feline radius and ulna. Vet Surg 2016; 45: 289-294
6. Witsberger TH, Hulse DA, Kerwin SC, Saunders WB. Minimally invasive application of a radial plate following placement of an ulnar rod in treating antebrachial fractures. Vet Comp Orthop Traumatol 2010; 23: 459-467
7. Grundnes O, Reikeras O. The importance of the hematoma for fracture healing in rats. Acta Orthopaedica Scandinavica 1993; 64: 340-342
8. Pozzi A, Risselada M, Winter MD. Assessment of fracture healing after minimally invasive plate osteosynthesis or open reduction and internal fixation of coexisting radius and ulna fractures in dogs via ultrasonography and radiography. J Am Vet Med Assoc 2012; 24: 744-753
9. Pozzi A, Hudson CC, Gauthier CM, Lewis DD. Retrospective comparison of minimally invasive plate osteosynthesis and open reduction and internal fixation of radius-ulna fractures in dogs. Vet Surg 2013; 42: 19-27
10. Rettig ME, Raskin KB. Galeazzi fracture-dislocation: A new treatment-oriented classification. J Hand Surg 2001; 26: 228-235
11. Sandness BM, Perry KL, Bruce M. Single institution retrospective study evaluating the frequency of implant removal and associated risk factors following open fracture fixation in 80 cases (2010-2020). BMC Vet Res 2023; 19; 119