

Novel dynamic screw-suture stabilization system for syndesmotic repair provides better anteroposterior translation and axial tibiofibular joint stability – a biomechanical investigation
Introduction
The quest for optimal treatment of acute distal tibiofibular syndesmotic disruptions is still in full progress. Using suture-button repair devices is one of the dynamic stabilization options; however, they may not be always appropriate for stabilization of length-unstable syndesmotic injuries. Recently, a novel screw-suture repair system was developed to address such issues (Fig 1). This implant system provides the fixation of a screw and the flexibility of a suture, addresses the limitations of suture-button constructs related to both the lack of tension control and medial soft-tissue disruption, and enables precise anatomical syndesmotic fixation.
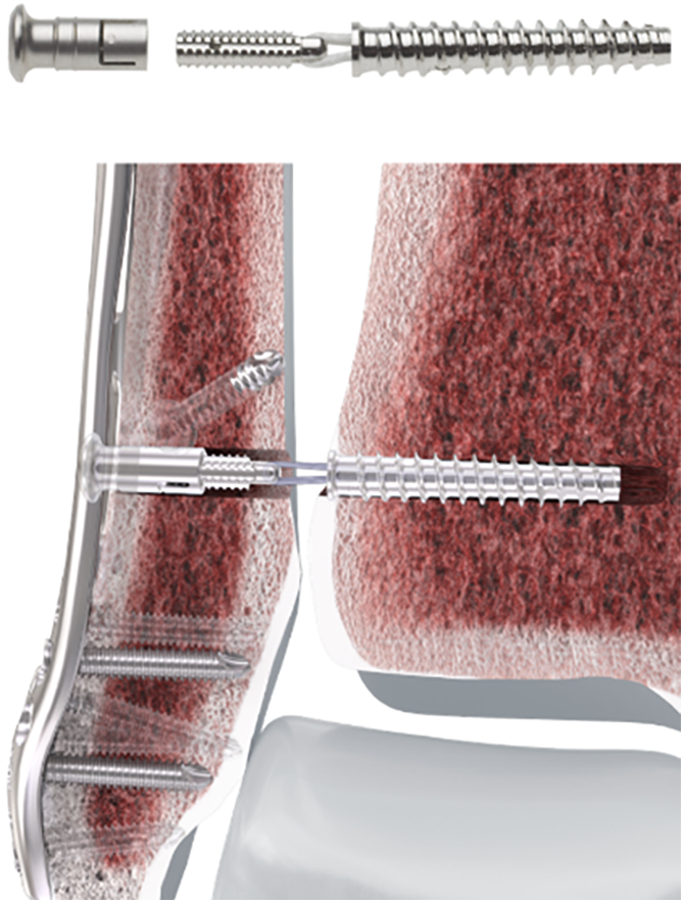
Fig 1 The novel screw-suture repair system for precise anatomical syndesmotic fixation.
The aim of this project was to investigate its performance compared with a suture-button stabilization of unstable syndesmotic injuries.
Materials and Methods
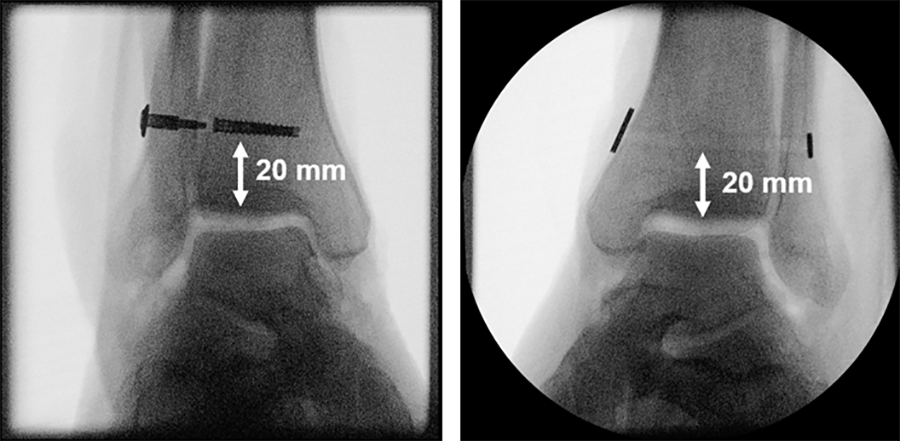
Eight pairs of human anatomical specimens, namely lower legs, were scanned by computed tomography (CT) under 700 N single-leg axial loading in five foot positions – neutral, 15° external/internal rotation and 20° dorsiflexion/plantarflexion in three different states: (1) pre-injury (intact); (2) injured, characterized by complete syndesmosis and deltoid ligaments cuts simulating pronation-eversion injury types III and IV as well as supination-eversion injury type IV according to Lauge-Hansen; (3) reconstructed, using a screw-suture (FIBULINK, Group 1) or a suture-button (TightRope, Group 2) implant for syndesmotic stabilization, placed 20 mm proximal to the tibia plafond/joint surface (Fig 2).
Next, all specimens were biomechanically tested over 5000 cycles under combined 1400 N axial and ±15° torsional loading. Clear space (diastasis), anterior tibiofibular distance, talar dome angle, and fibular shortening were measured radiologically from the CT scans. Anteroposterior, axial, mediolateral, and torsional movements at the distal tibiofibular joint level were evaluated biomechanically via motion tracking.
Results
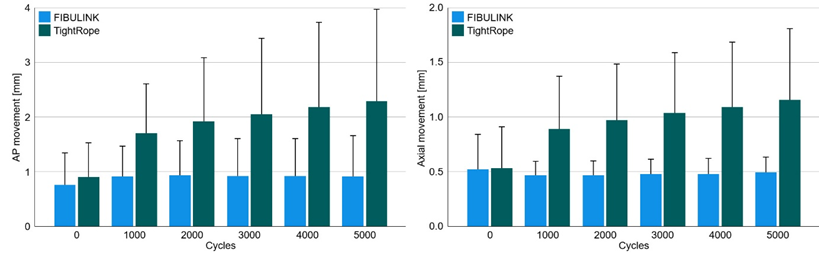
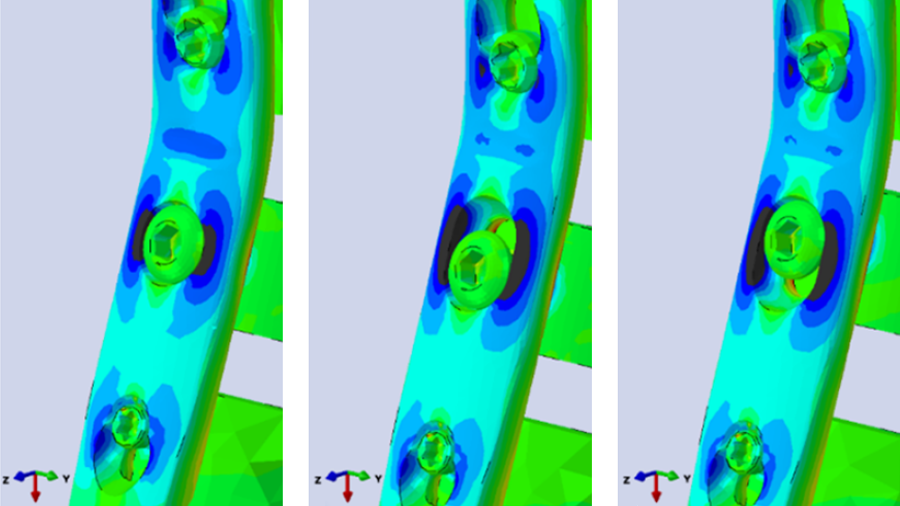
In each group clear space increased significantly after injury (P ≤ .004) and became significantly smaller in reconstructed compared with both pre-injured and injured states (P ≤ .041). In addition, after reconstruction it was significantly smaller in Group 1 compared with Group 2 (P < .001). Anteroposterior and axial movements were significantly smaller in Group 1 compared with Group 2 (P < .001; Fig 3). No further significant differences were identified nor detected between the two groups (P ≥ .113).
Conclusion
Although both implant systems demonstrate ability for stabilization of unstable syndesmotic injuries, the screw-suture reconstruction provides better anteroposterior translation and axial stability of the tibiofibular joint and maintains it over time under dynamic loading. Therefore, it can be considered as a valid option for treatment of syndesmotic disruptions.
You might also be interested in
-

FIBULINK Syndesmosis Repair System
The first adjustable syndesmotic repair system to enable precise, anatomical syndesmotic fixation.
-

Locked lateral plating vs. tension band wiring in patella fractures
Investigating the biomechanical performance of the two methods used for fixation of simple and complex patella fractures.
-
Helical plating
Provides well-balanced load sharing in laterally plated femoral defect fractures.
-
Pancarpal arthrodesis in canine
Although oval radiocarpal holes provide more options, they increase predicted failure risk.