

Acetabular bone defects: classification and diagnosis
Preview
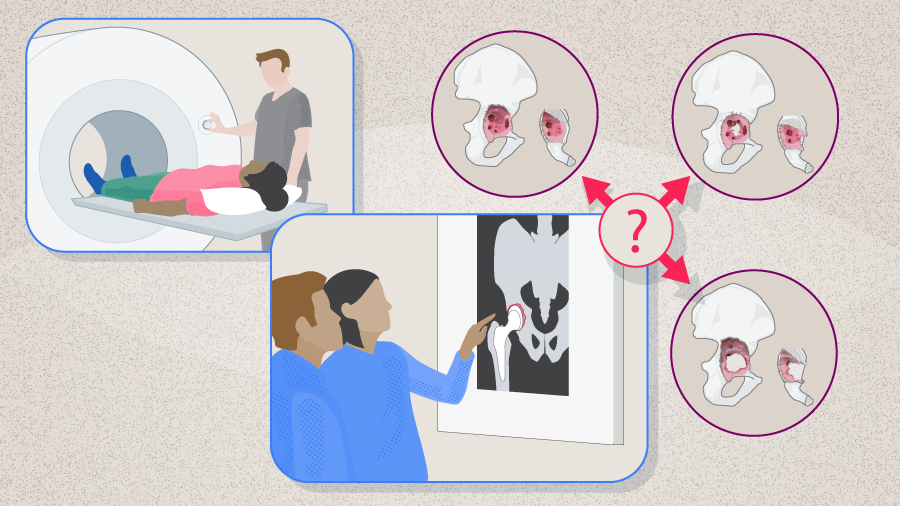
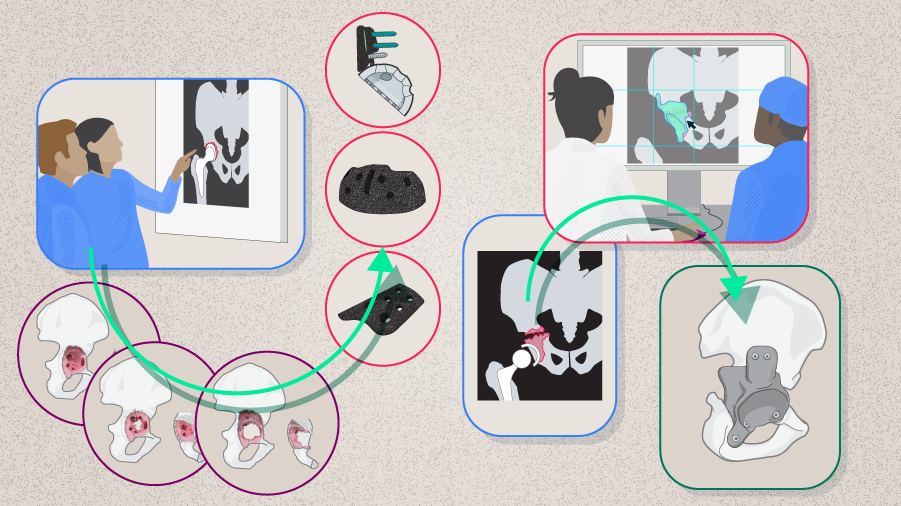
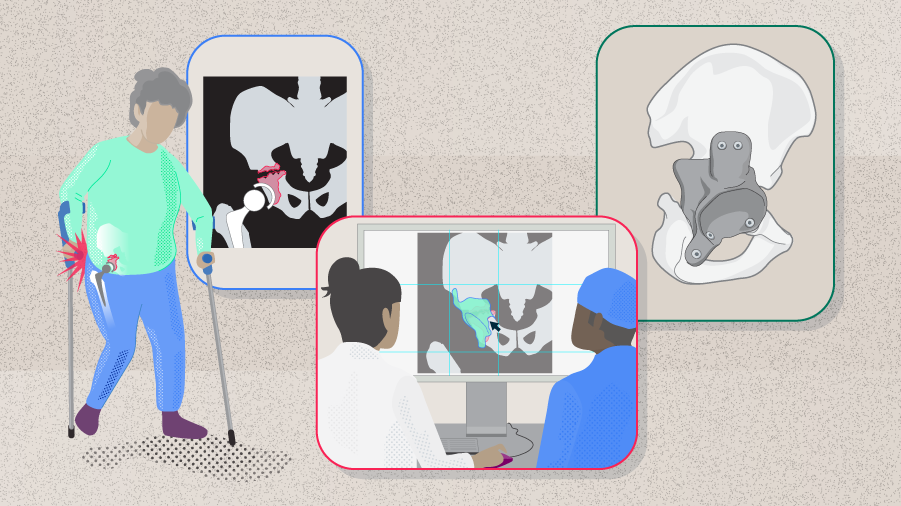
Failure of the acetabular component of a total hip arthroplasty (THA) is frequently associated with bone loss as a result of loosening and osteolysis; it is likely that bone defects will be extended during implant removal. The amount and location of acetabular bone loss greatly influence the degree of technical difficulty of revision THA (rTHA) [1]. An accurate preoperative assessment of the bone defect is therefore extremely important for surgical planning and successful outcomes, with the ultimate goal to conserve bone stock and reconstruct bone defects to ensure the longevity of the revision. In the first part of this series of articles, Thomas Kostakos from the Henry Dunant Medical Center, Athens, Hellenic Republic (Greece), will explain the importance of acetabular bone loss estimation along with the existing classification systems and the methods employed for a diagnosis.
Several classification systems have been published: the American Academy of Orthopaedic Surgeons (AAOS) [2], Paprosky [1], Gustilo [3], Engh [4], Gross [5], Saleh [6], and Parry [7] systems. The AAOS and Paprosky systems have been most widely used in the orthopedic community; these two systems are explained in the following sections.

Thomas Kostakos
Henry Dunant Medical Center, Athens, Greece
AAOS classification
The AAOS classification (Table 1) divides acetabular deficiencies into two basic categories: segmental and cavitary defects [2]. The cavitary defects represent a loss in volume of the acetabular bone without compromising the acetabular rim, while segmental defects involve the complete loss of acetabular bony structural support for the prosthesis [2].
The AAOS classification is widely used. Despite that, it does not address the magnitude of the defects, nor does it shed light on the specific management options of the defects [8–10]. In addition, this classification system was deemed to have low to moderate reliability and its validity has not been well established [9, 11].
Read the full article with your AO login
- AAOS classification
- Paprosky Classification
- Preoperative assessments
- Radiologial evaluation for bone quality information
- Hierarchical approach to preoperative imaging
- Current classification limitations
- When to engage CT
- Magnetic resonance imaging
- Conclusion
AO Recon resources
Contributing experts
This series of articles was created with the support of the following specialists (in alphabetical order):

Theofilos Karachalios
University General Hospital of Larissa at the University of Thessaly, Larissa, Greece
Thomas Kostakos
Henry Dunant Medical Center, Athens, Greece

George A Macheras
Henry Dunant Medical Center, Athens, Greece
The authors thank Maio Chen, medical writer at AO Innovation Translation Center, Switzerland, for contributing to the writing and editing of the articles.
References
- Paprosky WG, Perona PG, Lawrence JM. Acetabular defect classification and surgical reconstruction in revision arthroplasty. A 6-year follow-up evaluation. J Arthroplasty. 1994 Feb;9(1):33–44.
- D'Antonio JA, Capello WN, Borden LS, et al. Classification and management of acetabular abnormalities in total hip arthroplasty. Clin Orthop Relat Res. 1989 Jun(243):126–137.
- Gustilo RB, Pasternak HS. Revision total hip arthroplasty with titanium ingrowth prosthesis and bone grafting for failed cemented femoral component loosening. Clin Orthop Relat Res. 1988 Oct(235):111–119.
- Engh CA GA. Cementless revision of failed total hip replacement: an update. Instr Course Lect. 1991;40:189–197.
- Gross AE, Duncan CP, Garbuz D, Mohamed EM. Revision arthroplasty of the acetabulum in association with loss of bone stock. Instr Course Lect. 1999;48:57–66.
- Saleh KJ, Holtzman J, Gafni AL, et al. Development, test reliability and validation of a classification for revision hip arthroplasty. J Orthop Res. 2001 Jan;19(1):50–56.
- Parry MC, Whitehouse MR, Mehendale SA, et al. A comparison of the validity and reliability of established bone stock loss classification systems and the proposal of a novel classification system. Hip Int. 2010 Jan-Mar;20(1):50–55.
- Mancino F, Cacciola G, Di Matteo V, et al. Reconstruction options and outcomes for acetabular bone loss in revision hip arthroplasty. Orthop Rev (Pavia). 2020 Jun 29;12(Suppl 1):8655.
- Gu A, Adriani M, Malahias MA, et al. Reliability and Validity of Acetabular and Femoral Bone Loss Classification Systems in Total Hip Arthroplasty: A Systematic Review. HSS J. 2020 Oct;16(3):288–295.
- Sporer SM, O'Rourke M, Paprosky WG. The treatment of pelvic discontinuity during acetabular revision. J Arthroplasty. 2005 Jun;20(4 Suppl 2):79–84.
- Ghanem M, Zajonz D, Heyde CE, Roth A. Acetabular defect classification and management : Revision arthroplasty of the acetabular cup based on 3-point fixation. Orthopade. 2020 May;49(5):432–442.
- Neri T, Boyer B, Batailler C, et al. Dual mobility cups for total hip arthroplasty: tips and tricks. Sicot j. 2020;6:17.
- Sculco PK, Wright T, Malahias MA, et al. The Diagnosis and Treatment of Acetabular Bone Loss in Revision Hip Arthroplasty: An International Consensus Symposium. HSS J. 2022 Feb;18(1):8–41.
- Yu R, Hofstaetter JG, Sullivan T, et al. Validity and reliability of the Paprosky acetabular defect classification. Clin Orthop Relat Res. 2013 Jul;471(7):2259–2265.
- Babis GC, Nikolaou VS. Pelvic discontinuity: a challenge to overcome. EFORT Open Rev. 2021 Jun;6(6):459–471.
- Gozzard C, Blom A, Taylor A, et al. A comparison of the reliability and validity of bone stock loss classification systems used for revision hip surgery. J Arthroplasty. 2003 Aug;18(5):638–642.