

Overcoming surgical challenges in total hip arthroplasty in dysplastic high-riding hips
Preview
Developmental dysplasia of the hip (DDH) is the most common congenital disease of the musculoskeletal system in newborns [1]. If left untreated, limping can occur starting at walking age and premature hip arthritis can occur with severe osteoarthritis detected by the second decade [1, 2]. Severe cases of DDH-related arthritis are more frequently seen in Asia than in the US and Europe, probably because infant screening programs in the US and Europe are more prevalent [3]. The severity of DDH can vary from a subtle dysplasia to mild subluxation to complete dislocation. Due to the highly deformed femur and pelvis, performing total hip arthroplasty (THA) in severe cases of DDH is technically challenging; the complication rate can be high and the survivorship of the implants can be low. In Part 1 of this series, Seung Beom Han from the Department of Orthopedics, Korea University Medical Center, Seoul, South Korea, will discuss what the current practices are in performing THAs in highly deformed, high-riding hips.

Seung Beom Han
Department of Orthopedics
Korea University Medical Center
Seoul, South Korea
Classification of dysplastic hips
Crowe's classification system is the most used system in adult DDH, although the newer system described by Hartofilakidis et al [6] is also a reliable and commonly used system [2–6].
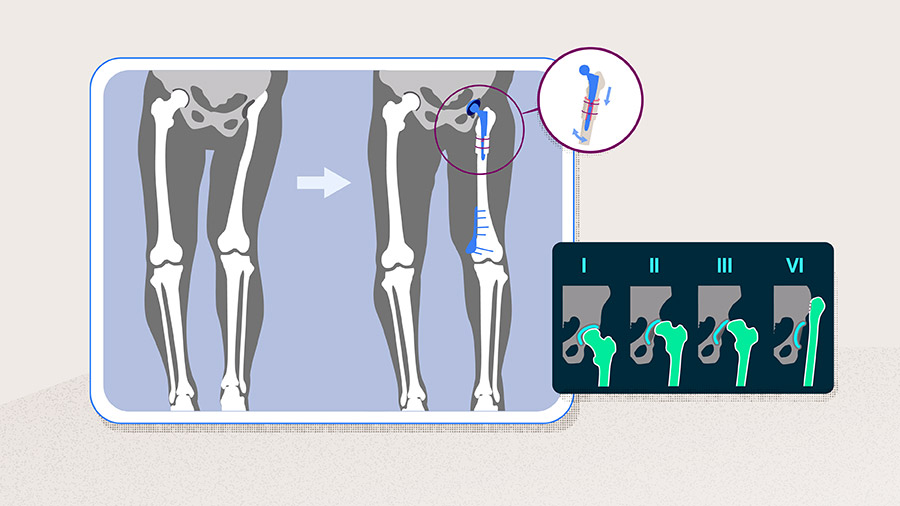
Crowe et al [7], based on their understanding that the degree of difficulty of THAs is associated with the severity of the dislocation and the subsequent distortion of normal bone and soft-tissue anatomy, grouped the dysplastic hips into four types based on the amount of dislocation (subluxation): < 50% in type I, 50–75% in type II, 75–100% in type III, and more than 100% in type IV.
As shown in Figure 1, the amount of deformity in DDH can progress from mild subluxation with a shallow socket (type I) to high dislocation of the hip joint accompanied by an absence of the femoral head and neck and a deformed pelvis (type IV). While a THA in DDH where subluxation is less than 50% has "no greater technical difficulty at surgery than a hip with severe osteoarthritis" [7], THAs in highly deformed DDHs are challenging and require special skills and consideration [2, 7].

The Hartofilakidis classification divides DDH into three types: A) dysplasia, B) low dislocation, and C) high dislocation (Table 1).
Read the full article with your AO login
- Three main challenges
- Treatment considerations
- Identification of the true acetabulum and acetabular component fixation
- Femoral deformity
- Bringing the high dislocation femoral head down to the true acetabulum
- Performing a subtrochanteric osteotomy
- Outcomes
- Conclusion
Additional AO resources
Access videos, tools, and other assets.
- Videos
- Upcoming events: AO Recon Course finder
Contributing experts
This series of articles was created with the support of the following specialists (in alphabetical order):
Seung Beom Han
Department of Orthopedics
Korea University Medical Center
Seoul, South Korea

Seung-Jae Lim
Department of Orthopedic Surgery
Samsung Medical Center
Seoul, South Korea
Youn-Soo Park
AO Recon Education Forum
Department of Orthopedic Surgery
Samsung Medical Center
Seoul, South Korea
This issue was written by Maio Chen, AO Innovation Translation Center, Clinical Science, Switzerland.
References
- Agostiniani R, Atti G, Bonforte S, et al. Recommendations for early diagnosis of Developmental Dysplasia of the Hip (DDH): working group intersociety consensus document. Italian Journal of Pediatrics. 2020 2020/10/09;46(1):150.
- Wang C, Ouyang Y, Liu H, et al. Surgery simulation teaching based on real reconstruction aid versus traditional surgical live teaching in the acquisition of an adult total hip arthroplasty surgical technique for developmental dysplasia of the hip: a randomized comparative study. BMC Medical Education. 2020 2020/07/20;20(1):228.
- Gustke K. The dysplastic hip: not for the shallow surgeon. Bone Joint J. 2013 Nov;95-b(11 Suppl A):31–36.
- Zhu J, Fernando ND. Classifications in Brief: The Hartofilakidis Classification of Developmental Dysplasia of the Hip. Clin Orthop Relat Res. 2020 Jan;478(1):189–194.
- Jawad MU, Scully SP. In brief: Crowe's classification: arthroplasty in developmental dysplasia of the hip. Clin Orthop Relat Res. 2011 Jan;469(1):306–308.
- Hartofilakidis G, Stamos K, Karachalios T, et al. Congenital hip disease in adults. Classification of acetabular deficiencies and operative treatment with acetabuloplasty combined with total hip arthroplasty. J Bone Joint Surg Am. 1996 May;78(5):683–692.
- Crowe JF, Mani VJ, Ranawat CS. Total hip replacement in congenital dislocation and dysplasia of the hip. J Bone Joint Surg Am. 1979 Jan;61(1):15–23.
- Chen M, Luo Z, Zhu C, et al. A Reliable Femoral Osteotomy in Total Hip Arthroplasty for Hartofilakidis Type C Developmental Dysplasia of the Hip: Proximal Femoral Reconstruction. J Arthroplasty. 2019 Jun;34(6):1162–1167.
- Wang D, Li LL, Wang HY, et al. Long-Term Results of Cementless Total Hip Arthroplasty With Subtrochanteric Shortening Osteotomy in Crowe Type IV Developmental Dysplasia. J Arthroplasty. 2017 Apr;32(4):1211–1219.
- Hartofilakidis G, Stamos K, Ioannidis T. Low friction arthroplasty for old untreated congenital dislocation of the hip. The Journal of Bone & Joint Surgery British Volume. 1988;70-B(2):182–186.
- Shi XT, Li CF, Han Y, et al. Total Hip Arthroplasty for Crowe Type IV Hip Dysplasia: Surgical Techniques and Postoperative Complications. Orthop Surg. 2019 Dec;11(6):966–973.
- Papachristou GC, Pappa E, Chytas D, et al. Total Hip Replacement in Developmental Hip Dysplasia: A Narrative Review. Cureus. 2021 Apr 29;13(4):e14763.
- Demirkale İ, Yaradılmış YU, Ateş A, et al. Total hip arthroplasty for high-riding hips: A retrospective analysis of 79 cases and proposal of a new classification. Journal of Orthopaedic Surgery. 2020 2020/05/01;28(2):2309499020924164.
- Charity JA, Tsiridis E, Sheeraz A, et al. Treatment of Crowe IV high hip dysplasia with total hip replacement using the Exeter stem and shortening derotational subtrochanteric osteotomy. J Bone Joint Surg Br. 2011 Jan;93(1):34–38.
- Shi XT, Li CF, Cheng CM, et al. Preoperative Planning for Total Hip Arthroplasty for Neglected Developmental Dysplasia of the Hip. Orthop Surg. 2019 Jun;11(3):348–355.
- Zhu B, Su C, He Y, et al. Combined anteversion technique in total hip arthroplasty for Crowe IV developmental dysplasia of the hip. Hip Int. 2017 Nov 21;27(6):589–594.
- Sentuerk U, von Roth P, Perka C. Ceramic on ceramic arthroplasty of the hip: new materials confirm appropriate use in young patients. Bone Joint J. 2016 Jan;98-b(1 Suppl A):14–17.
- Li C, Zhang C, Zhang M, et al. Comparison of transverse and modified subtrochanteric femoral shortening osteotomy in total hip arthroplasty for developmental dysplasia of hip: a meta-analysis. BMC Musculoskelet Disord. 2014 Oct 3;15:331.
- Muratli KS, Karatosun V, Uzun B, et al. Subtrochanteric shortening in total hip arthroplasty: biomechanical comparison of four techniques. J Arthroplasty. 2014 Apr;29(4):836–842.
- Lai KA, Shen WJ, Huang LW, et al. Cementless total hip arthroplasty and limb-length equalization in patients with unilateral Crowe type-IV hip dislocation. J Bone Joint Surg Am. 2005 Feb;87(2):339–345.
- Liu T, Wang S, Huang G, et al. Treatment of Crowe IV developmental dysplasia of the hip with cementless total hip arthroplasty and shortening subtrochanteric osteotomy. J Int Med Res. 2019 Jul;47(7):3223–3233.
- Caylak R, Ors C, Togrul E. Minimum 10-Year Results of Cementless Ceramic-On-Ceramic Total Hip Arthroplasty Performed With Transverse Subtrochanteric Osteotomy in Crowe Type IV Hips. J Arthroplasty. 2021 Oct;36(10):3519–3526.
- Sukur E, Senel A, Ozdemir U, et al. Cementless modular total hip arthroplasty with subtrochanteric transverse shortening osteotomy for high hip dislocations. Journal of Orthopaedic Surgery and Research. 2022 2022/03/04;17(1):139.
- Rollo G, Solarino G, Vicenti G, et al. Subtrochanteric femoral shortening osteotomy combined with cementless total hip replacement for Crowe type IV developmental dysplasia: a retrospective study. Journal of Orthopaedics and Traumatology. 2017 2017/12/01;18(4):407–413.
- Wang D, Li D-H, Li Q, et al. Subtrochanteric shortening osteotomy during cementless total hip arthroplasty in young patients with severe developmental dysplasia of the hip. BMC Musculoskeletal Disorders. 2017 2017/11/25;18(1):491.