

Extensor tendon rupture after total knee arthroplasty
Preview
Etiology
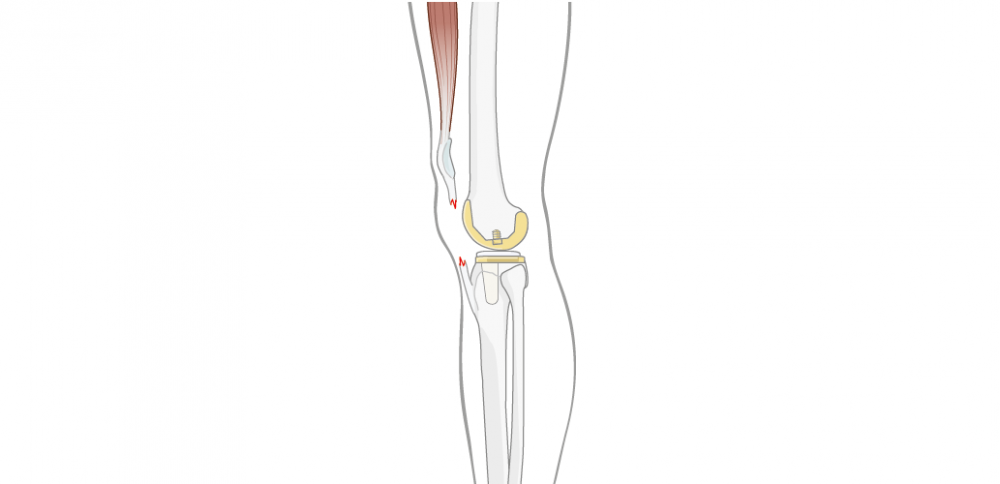
The incidence of extensor tendon rupture (Figure 1) after TKA has been reported in a range of 1–12% [1, 2]. Their etiology is complex and multifactorial, and poor results emphasize the importance of prevention [3–5]. Often, the rupture occurs during a traumatic event, which may be obvious, eg, a fall on the flexed knee, or trivial, eg, arising from a chair or carrying a heavy weight. Usually, the event causes the rupture because of preexisting fragility in the tendon [6].
The underlying reasons can either be patient-related or structural factors. When patient-related factors are the cause, several years may elapse between the TKA and the tendon rupture. When structural factors are the cause, the rupture often occurs early in the recuperative period [7].
Patient factors include obesity and other comorbidities. Obesity will lead to higher loads on the extensor, which it may not be able to withstand. On the other hand, several systemic diseases have an effect on soft-tissue quality, be it through their impact on blood supply, or through triggering inflammatory processes. Many comorbidities have been implicated in extensor tendon ruptures, including hyperthyroidism, diabetes mellitus, rheumatoid arthritis (RA), connective tissue disorders like systemic lupus erythematosus, and chronic renal failure [6, 8]. Additionally, long-term high-dosage glucocorticoid or fluoroquinolone use, or repeated intraarticular glucocorticoid injections can weaken collagenous tissues, and thus predispose patients for tendon ruptures [3].
Structural factors are often related to prior knee surgeries. To maintain good tissue quality of the extensor tendons in the long run, an optimal blood supply is vital. However, multiple surgical interventions around the extensor mechanism, including distal realignment procedures, will weaken and contribute to reduction of the blood supply [8]. The more extensive the dissection, the higher the compromise of the vascularization.

Yixin Zhou
Beijing Jishuitan Hospital
Beijing, China
Yixin Zhou, Professor and Chairman of Department of Adult Reconstructive Surgery, Beijing Jishuitan Hospital, points out: “Patients with the known relevant comorbidities, with stiff knees and a weak extensor mechanism, as well as male patients over 40 with tendinopathy, should raise red flags for surgeons and make them doubly careful with every maneuver avoiding overtension of the extensor. It is obvious that an impairment of vascularization has deleterious effects on any patient. However, in patients suffering from these conditions, the risk of subsequent tendon failure is so much higher. Therefore, every effort should be undertaken to be as vascularization-sparing as possible.”
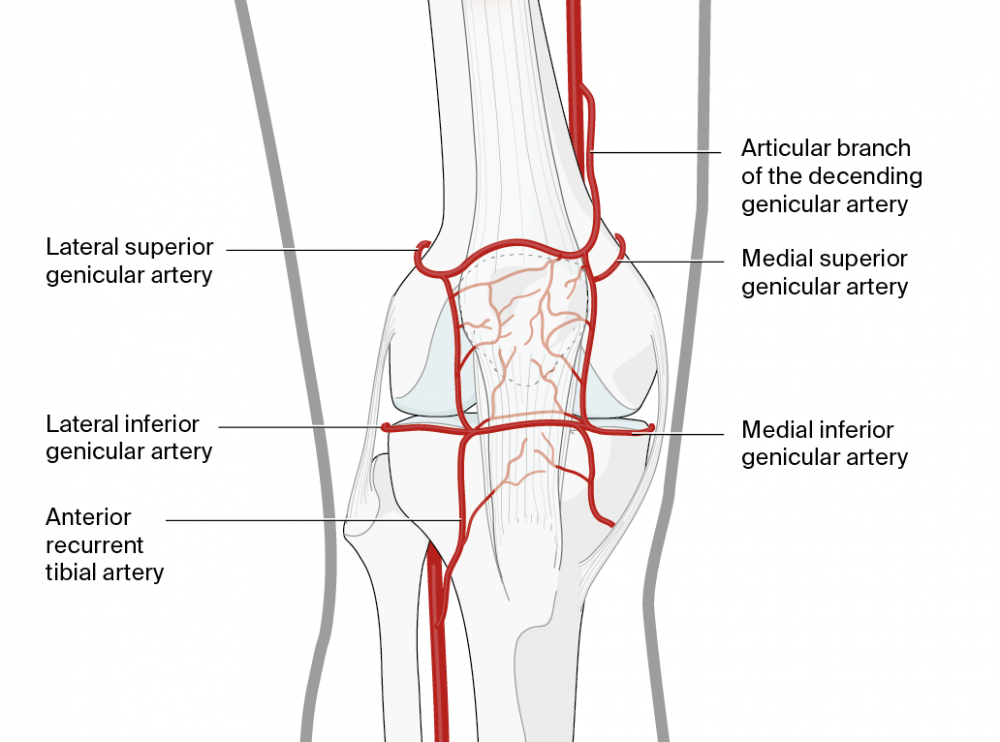
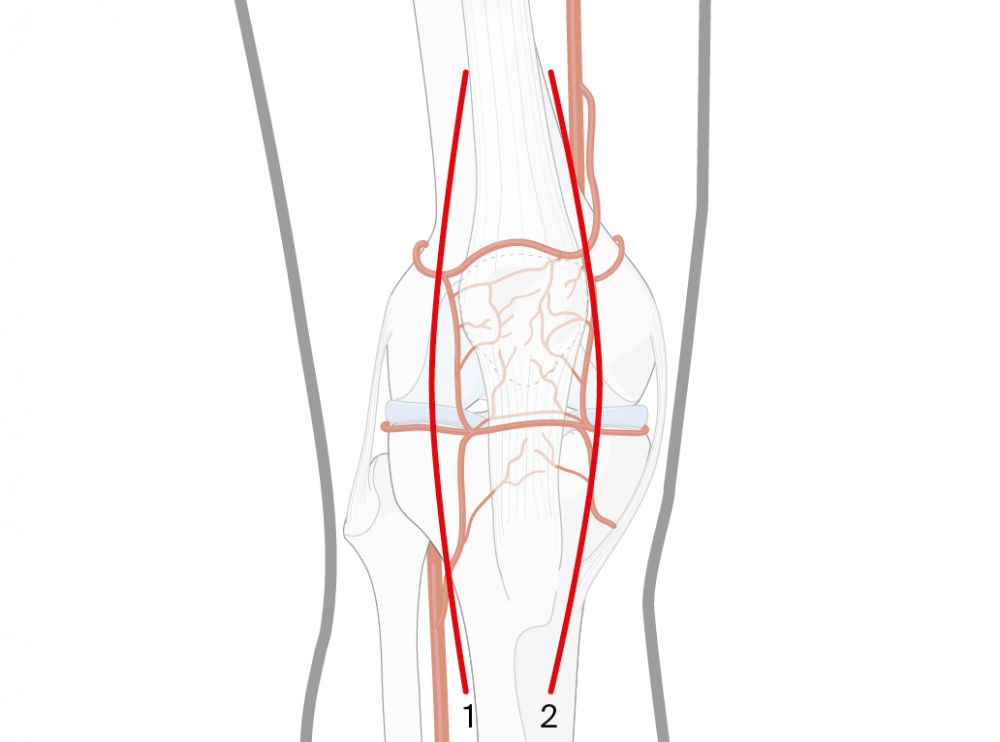
Upon performing the TKA surgery, various vascular structures are imperiled (Figure 2). First, the medial and descending genicular arteries are at risk during medial arthrotomy. Second, the lateral-inferior genicular artery and the anterior-tibial recurrent artery are at risk during fat-pad excision. Third, the lateral-superior genicular artery is at risk during release of the lateral retinaculum [6, 8–11].
Read the full article with your AO login
- The importance of tibiofemoral joint stability
- Surgical techniques
- Direct repair techniques
- Tendon reconstruction techniques
- Outcomes and conclusions


Additional AO resources on this topic
Access videos, tools, and other assets to learn more about this topic.
- Video: Extensor Mechanism Problems after Total Knee Arthroplasty
- Video: Managing Deformity in Total Knee Arthroplasty
- Video: The Difficult Primary Total Knee Arthroplasty
- Video: Tips and Tricks to Improve Total Knee Arthroplasty Outcomes
- Upcoming events: AO Recon Course finder
Contributing experts
This series of articles was created with the support of the following specialists (in alphabetical order):

Guillermo Bonilla
Fundación Santa Fe de Bogotá University Hospital
Bogotá, Colombia

Clemens Gwinner
Charité—University Medicine Berlin
Berlin, Germany
Yixin Zhou
Beijing Jishuitan Hospital
Beijing, China
This issue was written by Elke Rometsch, AO Innovation Translation Center, Clinical Science, Switzerland.
References
- Kelly MA. Patellofemoral complications following total knee arthroplasty. Instr Course Lect. 2001;50:403–407.
- Parker DA, Dunbar MJ, Rorabeck CH. Extensor mechanism failure associated with total knee arthroplasty: prevention and management. J Am Acad Orthop Surg. 2003 Jul-Aug;11(4):238–247.
- Dobbs RE, Hanssen AD, Lewallen DG, et al. Quadriceps tendon rupture after total knee arthroplasty. Prevalence, complications, and outcomes. J Bone Joint Surg Am. 2005 Jan;87(1):37–45.
- Healy WL, Wasilewski SA, Takei R, et al. Patellofemoral complications following total knee arthroplasty. Correlation with implant design and patient risk factors. J Arthroplasty. 1995 Apr;10(2):197–201.
- Rand JA, Morrey BF, Bryan RS. Patellar tendon rupture after total knee arthroplasty. Clin Orthop Relat Res. 1989 Jul(244):233–238.
- Bonnin M, Lustig S, Huten D. Extensor tendon ruptures after total knee arthroplasty. Orthop Traumatol Surg Res. 2016 Feb;102(1 Suppl):S21–31.
- Booth R, Jr. Extensor allograft: the consummate treatment for extensor disruption after total knee arthroplasty. Commentary on an article by Nicholas M. Brown, MD, et al: “Extensor mechanism allograft reconstruction for extensor mechanism failure following total knee arthroplasty”. J Bone Joint Surg Am. 2015 Feb 18;97(4):e25.
- Schoderbek RJ, Jr., Brown TE, Mulhall KJ, et al. Extensor mechanism disruption after total knee arthroplasty. Clin Orthop Relat Res. 2006 May;446:176–185.
- Nam D, Abdel MP, Cross MB, et al. The management of extensor mechanism complications in total knee arthroplasty. AAOS exhibit selection. J Bone Joint Surg Am. 2014 Mar 19;96(6):e47.
- Lynch AF, Rorabeck CH, Bourne RB. Extensor mechanism complications following total knee arthroplasty. J Arthroplasty. 1987;2(2):135–140.
- Pawar U, Rao KN, Sundaram PS, et al. Scintigraphic assessment of patellar viability in total knee arthroplasty after lateral release. J Arthroplasty. 2009 Jun;24(4):636–640.
- Emerson RH, Jr, Head WC, Malinin TI. Extensor mechanism reconstruction with an allograft after total knee arthroplasty. Clin Orthop Relat Res. 1994 Jun(303):79–85.
- Papalia R, Vasta S, D'Adamio S, et al. Complications involving the extensor mechanism after total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2015 Dec;23(12):3501–3515.
- Pagnano MW. Patellar tendon and quadriceps tendon tears after total knee arthroplasty. J Knee Surg. 2003 Oct;16(4):242–247.
- Kim TW, Kamath AF, Israelite CL. Suture anchor repair of quadriceps tendon rupture after total knee arthroplasty. J Arthroplasty. 2011 Aug;26(5):817–820.
- Krackow KA, Thomas SC, Jones LC. A new stitch for ligament-tendon fixation. Brief note. J Bone Joint Surg Am. 1986 Jun;68(5):764–766.
- Liu CC, Gao X, Xu M, et al. Surgical management of posterior knee dislocation associated with extensor apparatus rupture. Knee. 2017 Oct;24(5):940-948.
- Ode GE, Piasecki DP, Habet NA, et al. Cortical Button Fixation: A Better Patellar Tendon Repair? Am J Sports Med. 2016 Oct;44(10):2622–2628.
- Meyer Z, Ricci WM. Knee Extensor Mechanism Repairs: Standard Suture Repair and Novel Augmentation Technique. J Orthop Trauma. 2016 Aug;30 Suppl 2:S30–31.
- Rosenberg AG. Management of extensor mechanism rupture after TKA. J Bone Joint Surg Br. 2012 Nov;94(11 Suppl A):116–119.
- Jimenez A, Bedeir YH, Hasselfeld KA, et al. Novel repair of a quadriceps tendon rupture after a total knee arthroplasty using gracilis and semitendinosus autografts. Knee. 2020 Oct;27(5):1446–1450.
- Barrack RL, Stanley T, Allen Butler R. Treating extensor mechanism disruption after total knee arthroplasty. Clin Orthop Relat Res. 2003 Nov(416):98–104.
- Abdel MP, Salib CG, Mara KC, et al. Extensor Mechanism Reconstruction with Use of Marlex Mesh: A Series Study of 77 Total Knee Arthroplasties. J Bone Joint Surg Am. 2018 Aug 1;100(15):1309–1318.
- Browne JA, Hanssen AD. Reconstruction of patellar tendon disruption after total knee arthroplasty: results of a new technique utilizing synthetic mesh. J Bone Joint Surg Am. 2011 Jun 15;93(12):1137–1143.
- Hosey G, Kowalchick E, Tesoro D, et al. Comparison of the mechanical and histologic properties of Achilles tendons in New Zealand white rabbits secondarily repaired with Marlex mesh. J Foot Surg. 1991 May-Jun;30(3):214–233.
- Maffulli N, Del Buono A, Loppini M, et al. Ipsilateral hamstring tendon graft reconstruction for chronic patellar tendon ruptures: average 5.8-year follow-up. J Bone Joint Surg Am. 2013 Sep 4;95(17):e1231–1236.
- Järvelä T, Halonen P, Järvelä K, et al. Reconstruction of ruptured patellar tendon after total knee arthroplasty: a case report and a description of an alternative fixation method. Knee. 2005 Apr;12(2):139–143.
- Lamberti A, Balato G, Summa PP, et al. Surgical options for chronic patellar tendon rupture in total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2018 May;26(5):1429–1435.
- Aracil J, Salom M, Aroca JE, et al. Extensor apparatus reconstruction with Leeds-Keio ligament in total knee arthroplasty. J Arthroplasty. 1999 Feb;14(2):204–208.
- Ares O, Lozano LM, Medrano-Najera C, et al. New modified Achilles tendon allograft for treatment of chronic patellar tendon ruptures following total knee arthroplasty. Arch Orthop Trauma Surg. 2014 May;134(5):713–717.
- Fujikawa K, Ohtani T, Matsumoto H, et al. Reconstruction of the extensor apparatus of the knee with the Leeds-Keio ligament. J Bone Joint Surg Br. 1994 Mar;76(2):200–203.
- Pilge H, Holzapfel BM, Rechl H, et al. Function of the extensor mechanism of the knee after using the 'patellar-loop technique' to reconstruct the patellar tendon when replacing the proximal tibia for tumour. Bone Joint J. 2015 Aug;97-b(8):1063–1069.
- Cadambi A, Engh GA. Use of a semitendinosus tendon autogenous graft for rupture of the patellar ligament after total knee arthroplasty. A report of seven cases. J Bone Joint Surg Am. 1992 Aug;74(7):974–979.
- Donken CC, Caron JJ, Verhofstad MH. Functional reconstruction of a chronically ruptured extensor apparatus after patellectomy. J Knee Surg. 2009 Oct;22(4):378–381.
- Lim CT, Amanatullah DF, Huddleston JI, 3rd, et al. Reconstruction of Disrupted Extensor Mechanism After Total Knee Arthroplasty. J Arthroplasty. 2017 Oct;32(10):3134–3140.
- Wise BT, Erens G, Pour AE, et al. Long-term results of extensor mechanism reconstruction using Achilles tendon allograft after total knee arthroplasty. Int Orthop. 2018 Oct;42(10):2367–2373.
- Crossett LS, Sinha RK, Sechriest VF, et al. Reconstruction of a ruptured patellar tendon with achilles tendon allograft following total knee arthroplasty. J Bone Joint Surg Am. 2002 Aug;84(8):1354–1361.
- Diaz-Ledezma C, Orozco FR, Delasotta LA, et al. Extensor mechanism reconstruction with achilles tendon allograft in TKA: results of an abbreviate rehabilitation protocol. J Arthroplasty. 2014 Jun;29(6):1211–1215.
- Brown NM, Murray T, Sporer SM, et al. Extensor mechanism allograft reconstruction for extensor mechanism failure following total knee arthroplasty. J Bone Joint Surg Am. 2015 Feb 18;97(4):279–283.