


LCP Equine T-Plate 4.5
Christoph Lischer, Fabrice Rossignol, Jeffrey P Watkins
 Fig 1: Illustration of the 4-hole LCP Equine T-Plate 4.5 on a foal's tibia.
Fig 1: Illustration of the 4-hole LCP Equine T-Plate 4.5 on a foal's tibia. Physeal fractures of the foals proximal tibia are challenging cases to manage due to limited implant purchase in the small epiphyseal fracture segment and the relatively soft bone in the epiphysis and metaphysis. To avoid support limb complications in the active foals, they must return to full weightbearing on the affected limb immediately after surgery. Furthermore, the proximal location of the injury precludes the use of external coaptation to support the repair.
Currently, the recommended method of fixation is to use a standard plating technique, with a single screw in the proximal end of the plate engaging the epiphyseal segment. Single plate fixation is typically augmented with a transphyseal screw / wire fixation or, in large foals, a second plate.
The Equine T-Plate is designed to provide a single implant solution with multiple locking screw fixation in the epiphyseal segment as well as the ability to place locking screws throughout the length of the plate to augment fixation in the soft immature foal bone.
Plate design
The AOTK approved LCP Equine T-Plate 4.5 is indicated for the treatment of physeal fractures of the proximal tibia in foals. The plate is made of 316L stainless steel, is compatible with the Large Fragment system, and available in the following sizes (Fig 2):
- 4-hole plate (91 mm)
- 6-hole plate (127 mm)
- 8-hole plate (163 mm)
- 10-hole plate (199 mm)
The screw trajectory is designed to optimize bony purchase. Furthermore, cortex screws can be applied through the plate in lag fashion to compress the metaphyseal fracture common in type 2 physeal fractures of the proximal tibia in foals. Additional wire holes allow temporary fixation with K-wires in the epiphysis, and combi-holes allow cortex screw and locking screw fixation at the discretion of the surgeon (Figs 3 and 4):
- Stacked combi-holes in the head of the plate accept locking and cortex screws
- Standard combi-holes in the straight portion of the plate allow screw selection as well as the opportunity to provide dynamic compression between fracture segments with cortex screws
- Incorporation of locking technology permits a fixed-angle device to increase construct stability and augment fixation in soft, immature bone.
Versatility
The Equine T-Plate, which incorporates locking technology, is intended to enhance fixation in short fracture segments where traditional plate fixation would be inadequate. Although the plate has been designed to treat physeal fractures of the foals proximal tibia, there are a wide variety of other applications including physeal or metaphyseal fractures of other long bones as well as partial carpal and tarsal arthrodesis.
 Fig 2: Illustration of the LCP Equine T-Plate 4.5 portfolio.
Fig 2: Illustration of the LCP Equine T-Plate 4.5 portfolio. 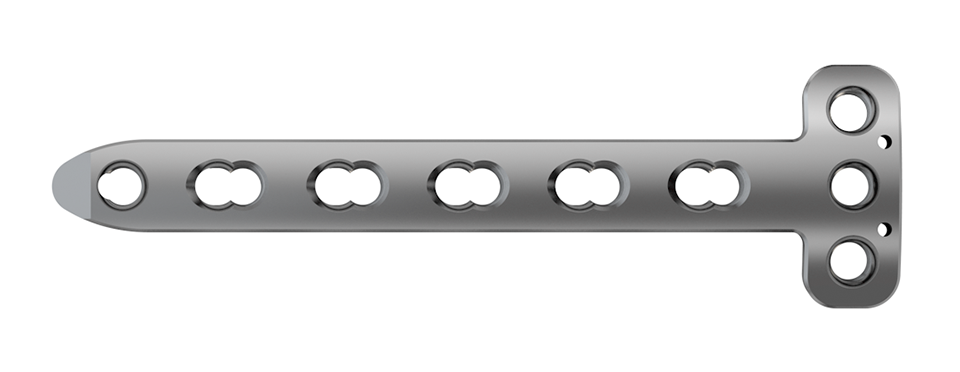 Fig 3: Top view of the 6-hole plate showing the stacked combi-holes and K-wire holes in the head of the plate. The straight portion of the plate features standard combi-holes and a single stacked combi-hole at the tip of the plate.
Fig 3: Top view of the 6-hole plate showing the stacked combi-holes and K-wire holes in the head of the plate. The straight portion of the plate features standard combi-holes and a single stacked combi-hole at the tip of the plate.  Fig 4: Side view of the Equine T-Plate indicating the screw trajectories (angulation of 5° inwards) in the precontoured head of the plate.
Fig 4: Side view of the Equine T-Plate indicating the screw trajectories (angulation of 5° inwards) in the precontoured head of the plate.
The two cases presented here demonstrate the utility of the Equine T-Plate to provide solid fixation in short fracture segments. Specifically, the T-portion of the plate can be used to engage up to 3 locking screws in fracture segments where standard plate fixation would be inadequate. In addition, case 2 also shows that even in neonatal bone, where the holding power of standard cortex screws can be a limitation, multiple locking screw fixation provides a strong, stable construct. Case 1 demonstrates that the Equine T-Plate has application in other locations, where fixation is limited by close proximity to a joint. Many additional indications exist where the ability to provide multiple locking screw fixation is limited by proximity to a joint or physis and the Equine T-Plate will provide a useful solution.
Case 1: Elective partial carpal arthrodesis in a warmblood broodmare
(Case provided by Fabrice Rossignol, Paris, France)
A 4-year-old French warmblood broodmare weighing 570 kg presented with a 5-day history of severe right forelimb lameness following an unwitnessed paddock accident. The limb had been stabilized in a Robert-Jones bandage with caudal and lateral splints prior to referral. The radiographs confirmed a slab fracture of the third carpal bone as well as a comminuted biarticular fracture of the fourth carpal bone (Fig 5). An arthrodesis of the carpometacarpal and middle carpal joint was elected.
The day after admission, the mare was placed under general anesthesia in dorsal recumbency for a partial carpal arthrodesis of the right carpometacarpal and middle carpal joints. The middle carpal joint was examined arthroscopically, and all visible articular cartilage was removed by using a combination of manual (bone curette) and motorized (shaver/burr) instrumentation (Fig 6). A 4.5 mm drill bit was used to drill across the carpometacarpal joint surfaces. A cancellous bone graft harvested from the sternum was loosely packed into the repair through an arthroscopic portal with the leg in flexion. Following graft insertion, implants were placed using a minimally invasive technique, tunneling the plate under the skin and joint capsule, and stab incisions for screw insertions. A 6-hole LCP Equine T-plate 4.5 was applied to the dorsal aspect of the limb deep to the extensor tendons and joint capsule through an enlarged arthroscopic portal between the extensor carpi radialis and common digital extensor tendon using a plate passer. A 4.5 mm cortex screw was placed in the first hole of the shaft of the plate to compress the plate to the bone. Two 5.0 mm locking screws were placed in the holes of the horizontal portion of the plate to engage the intermediate carpal bone. A third 5.0 mm locking screw was placed into the radial carpal bone using the last hole of the horizontal portion of the plate (Fig 7). All remaining holes were filled with 5.0 mm locking screws except the second hole, which was left empty because the hole was directly over the carpometacarpal joint. A 6-hole narrow LCP 4.5 was applied dorsolaterally and a 6-hole narrow LCP 4.5 was placed dorsomedially in a similar manner. The skin incisions were closed in routine fashion, and a sterile dressing and full limb cast were applied. The mare recovered uneventfully from anesthesia with head and tail assistance.
The cast was removed 24 hours postoperatively, and a Robert- Jones bandage with caudal and lateral splints was maintained for 1 month. The mare made excellent postoperative progress with immediate full weightbearing on the operated leg. At 5 months postoperatively, radiographic evaluation confirmed excellent healing of the fracture and almost complete fusion of the middle carpal and carpometacarpal joints with preservation of the radiocarpal joint (Fig 8). At one year postoperatively, the mare showed a very good cosmetic aspect of the carpus, as well as an excellent locomotion at three gates, with only minor mechanical lameness due to reduction of carpal flexion (Fig 9).
 Fig 5a-b: Preoperative radiographs: Dorsopalmar (DP) (a) and flexed dorsomedial-palmarolateral oblique (DMPLO) views (b).
Fig 5a-b: Preoperative radiographs: Dorsopalmar (DP) (a) and flexed dorsomedial-palmarolateral oblique (DMPLO) views (b).  Fig 6a-b: Arthroscopic cartilage removal by using motorized (shaver/burr) instrumentation.
Fig 6a-b: Arthroscopic cartilage removal by using motorized (shaver/burr) instrumentation.  Fig 7a-c: Postoperative radiographs: DP (a), dorsolateral-palmaromedial oblique (DLPMO) (b), and lateromedial (LM) (c) views.
Fig 7a-c: Postoperative radiographs: DP (a), dorsolateral-palmaromedial oblique (DLPMO) (b), and lateromedial (LM) (c) views.  Fig 8ac: Five-month postoperative radiographs: DLPMO (a), DP (b) and DMPLO (c) views.
Fig 8ac: Five-month postoperative radiographs: DLPMO (a), DP (b) and DMPLO (c) views.  Fig 9: Very good cosmetic aspect of the carpus at 5 months postoperative with partial degree of flexion.
Fig 9: Very good cosmetic aspect of the carpus at 5 months postoperative with partial degree of flexion.
Case 2: Complete distal radial fracture in a 4-hour old foal
(Case provided by Thijs de Bont, Brussels, Belgium)
A 68 kg Warmblood foal was presented for evaluation and treatment of a complete open fracture of the left distal radius sustained during parturition 4 hours earlier. The fracture had occurred when the mare laid down against the wall of the stables while the foal was partially through the birth canal. The foal had been recumbent since birth. The limb had been partially stabilized with a full limb bandage and lateral splint prior to admission. The radiographs confirmed the presence of a complete slightly oblique (proximomedial to distolateral) open fracture, just proximal of the distal radial physis (Fig 10). Extensive maceration of the medial soft tissues just proximal of the carpus was noted, with a 0.5 cm full thickness skin laceration. The foal was stabilized and was taken to surgery a few hours following admission.
The foal was anesthetized and placed in dorsal recumbency. The left forelimb was placed in extension, clipped, prepared, and draped for aseptic surgery. A cranial approach to the distal aspect of the radius was made. The fracture was reduced, and a 6-hole LCP Equine T-Plate 4.5 was placed beneath the extensor carpi radialis (Fig 11). Two 5.0 mm locking screws were placed in the horizontal portion of the plate to engage the distal portion of the radius, just proximal of the distal radial physis. A 4.5 mm cortex screw was then placed into the second hole of the shaft of the plate, to provide interfragmentary compression and compress the plate to the proximal portion of the bone. The remaining holes were filled with 5.0 mm locking screws. The presurgical planning had included placing a second lateral LCP plate, however, the foals physiological status deteriorated. Further fracture fixation was therefore abandoned, and the surgery site was closed. A tube cast was placed from the level of the fetlock to the proximal radius. The foot and pastern were left free to minimize flexor tendon laxity. The foal was placed in sternal recumbency and required 2 hours of assisted ventilation before she started to breath spontaneously. Following surgery, she stood unassisted and was able to ambulate and suckle.
The cast was changed every 7 days and was replaced with a two-layer full limb bandage 28 days postoperatively. Carpal hyperextension was counteracted with an elastic band taped to the palmar aspect of the limb under tension, to prevent hyperextension when the limb was loaded (Fig 12). Tensions were adjusted depending on the increasing weight and strength of the foal. Once the cast was removed, the foal was hand walked daily.
Postoperatively, the foal was noted to have a moderate carpus valgus deformity. Radiographic assessment, however, showed that the lateral deviation was not due to malalignment of the fracture. A gradual improvement in the degree of valgus deformity has been seen with growth as the foal has matured (Fig 13). Radiographic healing of the fracture has proceeded quickly with very little callus formation (Fig 14).
 Fig 10ad: Preoperative radiographs: LM (a), DP (b), DLPMO (c), and DMPLO (d) views.
Fig 10ad: Preoperative radiographs: LM (a), DP (b), DLPMO (c), and DMPLO (d) views.  Fig 11ad: Postoperative radiographs: LM (a), DP (b), DLPMO (c), and DMPLO (d) views.
Fig 11ad: Postoperative radiographs: LM (a), DP (b), DLPMO (c), and DMPLO (d) views.  Fig 12ab: Appearance of the limb following cast removal 28 days postoperatively before (a) and after (b) application of the palmar elastic.
Fig 12ab: Appearance of the limb following cast removal 28 days postoperatively before (a) and after (b) application of the palmar elastic.  Fig 13: Appearance of the limb 7 weeks following surgery.
Fig 13: Appearance of the limb 7 weeks following surgery. 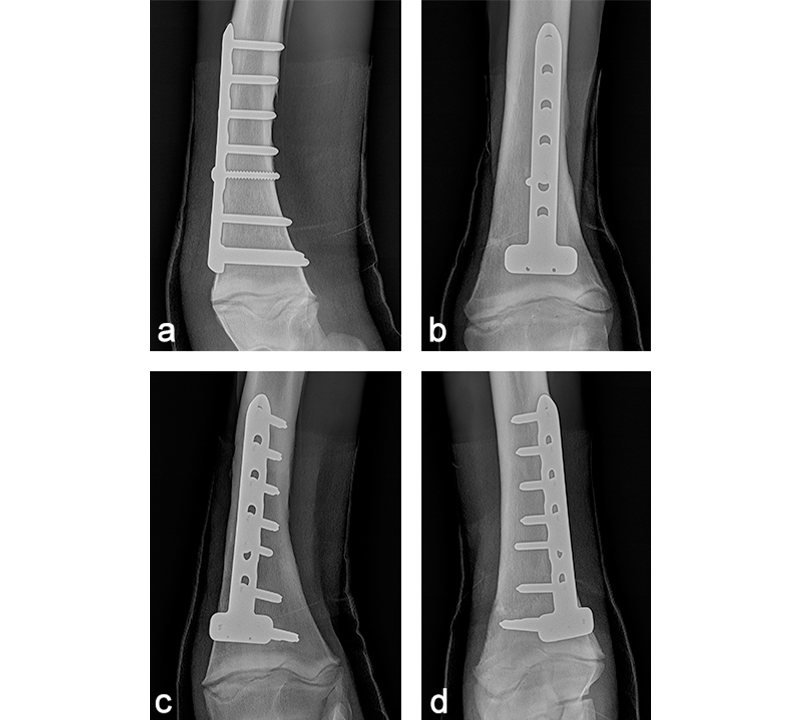 Fig 14a–d: Postoperative radiographs at 9 weeks: LM (a), DP (b), DLPMO (c), and DMPLO (d) views.
Fig 14a–d: Postoperative radiographs at 9 weeks: LM (a), DP (b), DLPMO (c), and DMPLO (d) views. LCP Equine T-Plate 4.5
Hazards and labeling
Due to varying countries’ legal and regulatory approval requirements, consult the appropriate local product labeling for approved intended use of the products described on this website. All devices on this website are approved by the AO Technical Commission. For logistical reasons, these devices may not be available in all countries worldwide at the date of publication.
Legal restrictions
This work was produced by AO Foundation, Switzerland. All rights reserved by AO Foundation. This publication, including all parts thereof, is legally protected by copyright.
Any use, exploitation or commercialization outside the narrow limits set forth by copyright legislation and the restrictions on use laid out below, without the publisher‘s consent, is illegal and liable to prosecution. This applies in particular to photostat reproduction, copying, scanning or duplication of any kind, translation, preparation of microfilms, electronic data processing, and storage such as making this publication available on Intranet or Internet.
Some of the products, names, instruments, treatments, logos, designs, etc referred to in this publication are also protected by patents, trademarks or by other intellectual property protection laws (eg, “AO” and the AO logo are subject to trademark applications/registrations) even though specific reference to this fact is not always made in the text. Therefore, the appearance of a name, instrument, etc without designation as proprietary is not to be construed as a representation by the publisher that it is in the public domain.
Restrictions on use: The rightful owner of an authorized copy of this work may use it for educational and research purposes only. Single images or illustrations may be copied for research or educational purposes only. The images or illustrations may not be altered in any way and need to carry the following statement of origin “Copyright by AO Foundation, Switzerland”.
Check www.aofoundation.org/disclaimer for more information.
If you have any comments or questions on the articles or the new devices, please do not hesitate to contact us.
“approved by AO Technical Commission” and “approved by AO”
The brands and labels “approved by AO Technical Commission” and “approved by AO”, particularly "AO" and the AO logo, are AO Foundation's intellectual property and subject to trademark applications and registrations, respectively. The use of these brands and labels is regulated by licensing agreements between AO Foundation and the producers of innovation products obliged to use such labels to declare the products as AO Technical Commission or AO Foundation approved solutions. Any unauthorized or inadequate use of these trademarks may be subject to legal action.

AO ITC Innovations Magazine
Find all issues of the AO ITC Innovations Magazine for download here.


Innovation Awards
Recognizing outstanding achievements in development and fostering excellence in surgical innovation.