


Biphasic Plate Distal Femur
Ladina Hofmann-Fliri, Devakar Epari, Markus Windolf, Christoph Sommer
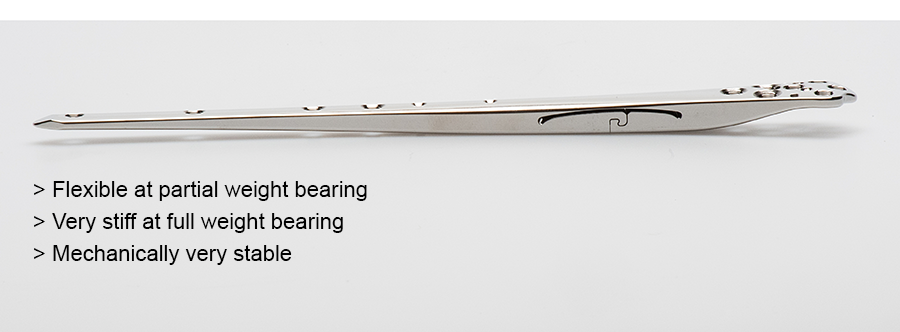 Fig 1: Biphasic Plate Distal Femur.
Fig 1: Biphasic Plate Distal Femur. Severe trauma to the extremities is a leading cause of disability during the wage-earning period. The socioeconomic burden of fracture is substantial. Loss of working capacity can account up to 50% of the total costs of the fracture [1]. Optimal outcomes require not only solid bone union but also early and complete recovery of limb function. The current generation of fracture fixation plates focuses on minimizing the impact of surgery and preserving the biological healing potential. However, their design poorly controls a second critical component—the mechanical environment of the fracture. Furthermore, these plates are prone to failure which limits function and delays return to work.
The Biphasic Plate (Fig 1) is designed to provide suitable flexibility for healing and increased implant strength to support early full weight bearing.
Clinical problem
Although distal femoral fractures account for approximately 3%–6% of all femoral fractures [2], they are challenging injuries, often complex, intraarticular, and comminuted in nature [3]. Open reduction and internal fixation (ORIF) with locking plate fixation is the most used treatment modality for distal femoral fractures but is associated with high incidence of complications [4]. A metaanalysis [5] reported a total reoperation rate of 13.6%, with nonunion (4.5%), mechanical failure (3.5%), and deep infection (3.2%) as the leading causes of reoperation.
Despite improvements in implant and technique, early full weight bearing after fixation is usually restricted due to concern of implant failure, and reduced weight bearing is recommended until radiographs indicate callus formation [6]. This is contrary to the preclinical evidence that callus formation is a product of interfragmentary motion [7]. Locking plates can inherently produce stiff constructs that have been known to suppress fracture healing [3, 8].
Biphasic plating is a new plating concept that was proposed by the AO Research Institute Davos (ARI) in collaboration with the Queensland University of Technology (QUT) in Brisbane, Australia, to enhance the existing treatment modalities of locked plating by redesigning the conventional bone plate. On April 21, 2021, the Biphasic Plate DF (Distal Femur) obtained the CE certification as a class IIB medical device. This achievement represents an impressive team effort, made possible by the Development Incubator funding of the AO ITC Technology Transfer.
Solution
The Biphasic Plate DF features a transverse slot in a region of increased plate thickness (Fig 2). This new plate design:
- Provides a beneficial and controlled mechanical environment at the fracture site for robust fracture healing (Fig 3)
- Increases implant strength which carries potential to permit full early weight bearing and prevent implant fatigue-related plate failure
- Standardizes; thus, simplifies the surgical procedure
Indications
The Biphasic Plate DF is indicated for the stabilization of distal femoral fractures, which include:
- Distal shaft fractures
- Supracondylar fractures
- Intraarticular fractures
- Periprosthetic fractures
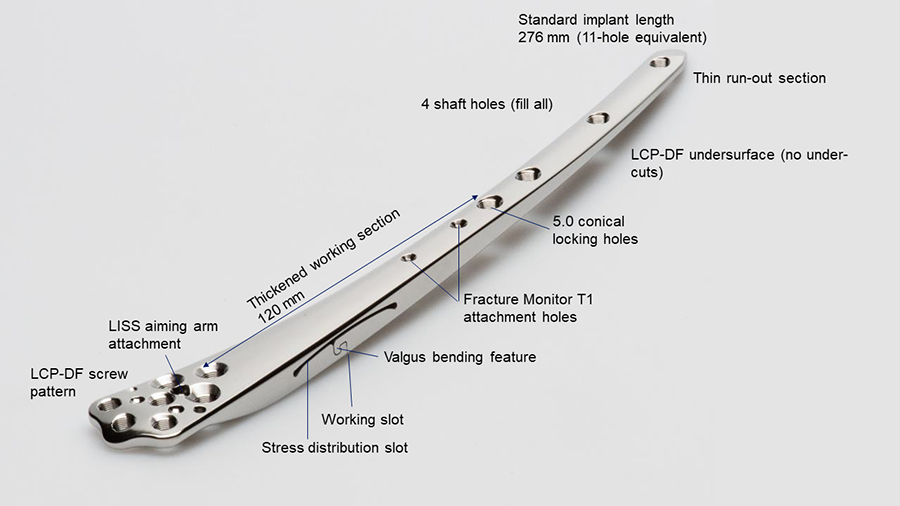 Fig 2: Features of the Biphasic Plate Distal Femur.
Fig 2: Features of the Biphasic Plate Distal Femur. 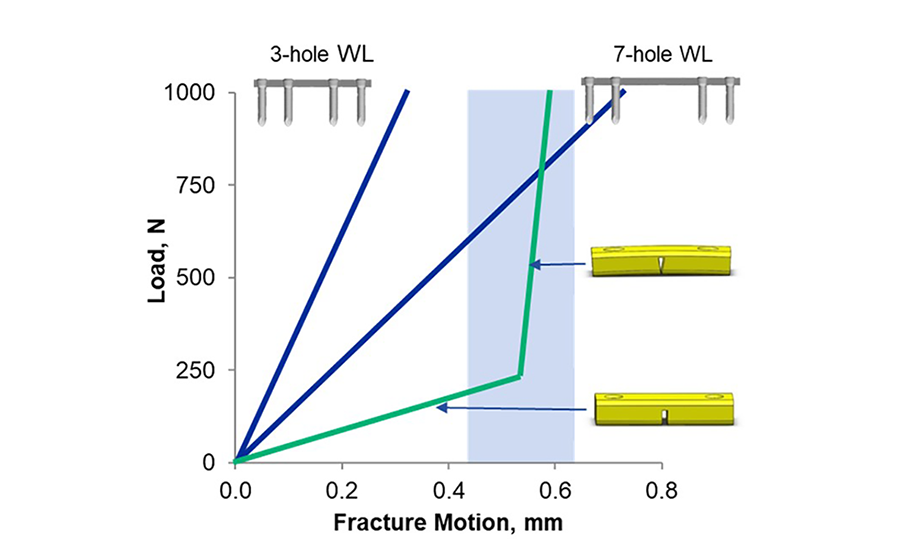 Fig 3: Standard locking plates produce variable fracture motion depending on the working length, whereas the Biphasic Plate provides controlled fracture motion over a wide load range. The light blue area represents the desired fracture gap motion for optimal bone healing.
Fig 3: Standard locking plates produce variable fracture motion depending on the working length, whereas the Biphasic Plate provides controlled fracture motion over a wide load range. The light blue area represents the desired fracture gap motion for optimal bone healing. Preclinical testing
Preclinical results confirmed the feasibility of the biphasic plating concept [9]. Sheep tibia osteotomies stabilized with a biphasic plate prototype showed robust callus formation without implant failure under various simulated fracture conditions [9]. A finite element analysis revealed that the biphasic plate exhibited a bilinear stiffness response; at low loads, the biphasic plate construct was 55% less stiff and at high loads 476% stiffer than the locking compression plate for the distal femur (LCP-DF) [10]. The biphasic plate provided more consistent interfragmentary movement over a wider loading range [10]. Subjected to dynamic loading, the LCP-DF failed on average after 322,369 cycles (standard deviation: 57,345), whereas none of the four tested biphasic plates showed any sign of failure at 1,000,000 cycles [11].
References
- Bonafede M, Espindle D, Bower AG. The direct and indirect costs of long bone fractures in a working age US population. J Med Econ. 2013 Feb;16(1):169−178.
- Court-Brown CM, Caesar B. Epidemiology of adult fractures: a review. Injury. 2006 Aug;37(8):691−697.
- Gangavalli AK, Nwachuku CO. Management of distal femur fractures in adults: an overview of options. Orthop Clin North Am. 2016 Jan;47(1):85−96.
- Henderson CE, Lujan TJ, Kuhl LL, et al. 2010 mid-America Orthopaedic Association Physician in Training Award: healing complications are common after locked plating for distal femur fractures. Clin Orthop Relat Res. 2011 Jun;469(6):1757−1765.
- Koso RE, Terhoeve C, Steen RG, et al. Healing, nonunion, and re-operation after internal fixation of diaphyseal and distal femoral fractures: a systematic review and meta-analysis. Int Orthop. 2018 Nov;42(11):2675−2683.
- Granata JD, Litsky AS, Lustenberger DP, et al. Immediate weight bearing of comminuted supracondylar femur fractures using locked plate fixation. Orthopedics. 2012 Aug 1;35(8):e1210−1213.
- Windolf M, Ernst M, Schwyn R, et al. A Biofeedback System for Continuous Monitoring of Bone Healing. Proceedings of the International Conference on Biomedical Electronics and Devices. 2014:243−248.
- Krieg JC. Locked plating of distal femur fractures leads to inconsistent and asymmetric callus formation. J Orthop Trauma. 2011 Feb;25(2):e21; author reply e21−22.
- Hofmann-Fliri L, Epari DR, Schwyn R, et al. Biphasic Plating: in vivo study of a novel fixation concept to enhance mechanobiological fracture healing. Injury. 2020 Aug;51(8):1751−1758.
- Epari DR, Gurung R, Hofmann-Fliri L, et al. Biphasic plating improves the mechanical performance of locked plating for distal femur fractures. J Biomech. 2021 Jan 22;115:110192.
- Roethlisberger S. Cyclic axial fatigue to compare the LCP-DF with the Biphasic Plate DF (Report No. A20_0595_4). RMS Foundation; 2020.
The Biphasic Plate DF is designed to be compatible with existing 5.0 mm DePuy Synthes locking screws (stainless steel) and insertion instruments for the LCP-DF.
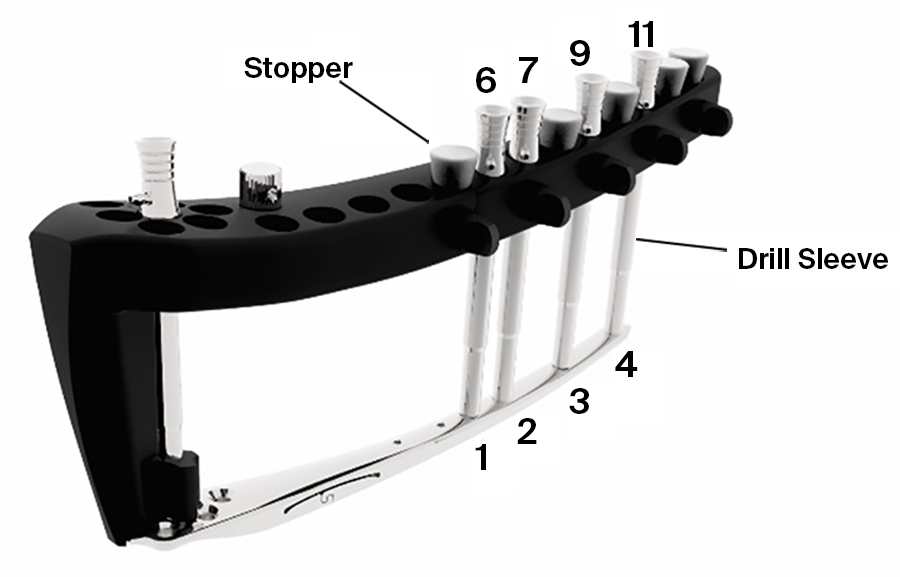 Fig 4: Biphasic Plate DF attached to the LISS Insertion Guide for Distal Femur.
Fig 4: Biphasic Plate DF attached to the LISS Insertion Guide for Distal Femur. Clinical cases from Christoph Sommer (Kantonsspital Graubünden, Chur, Switzerland)
Case 1
A 64-year-old man was involved in a car injury and sustained a complex floating knee injury with a comminuted distal femoral fracture and a proximal tibial fracture on the left side among various other fractures (Fig 5).
The distal femoral fracture was fixed 3 weeks after injury with ORIF and a Biphasic Plate DF (Fig 6).
The patient healed and returned to preoperative function (Fig 7).
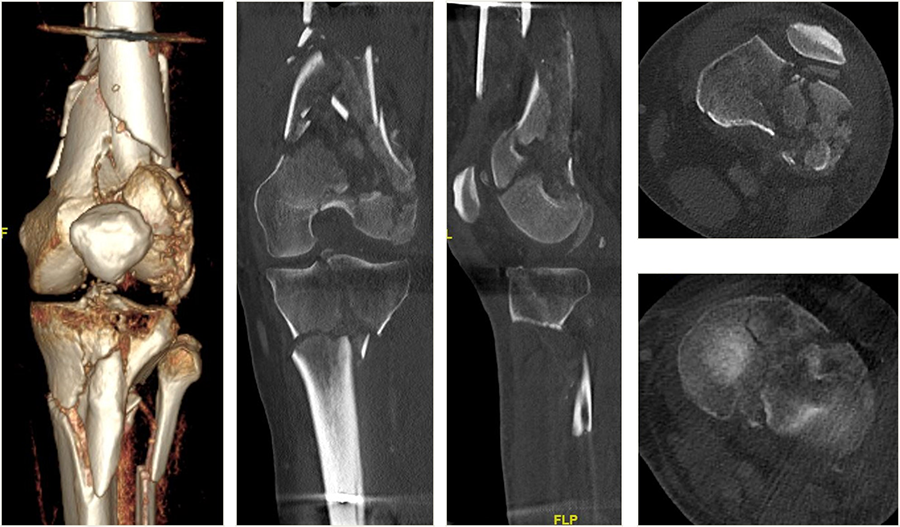 Fig 5: Computed tomographic scans and radiographs revealed the complex floating knee injury of the left leg.
Fig 5: Computed tomographic scans and radiographs revealed the complex floating knee injury of the left leg. 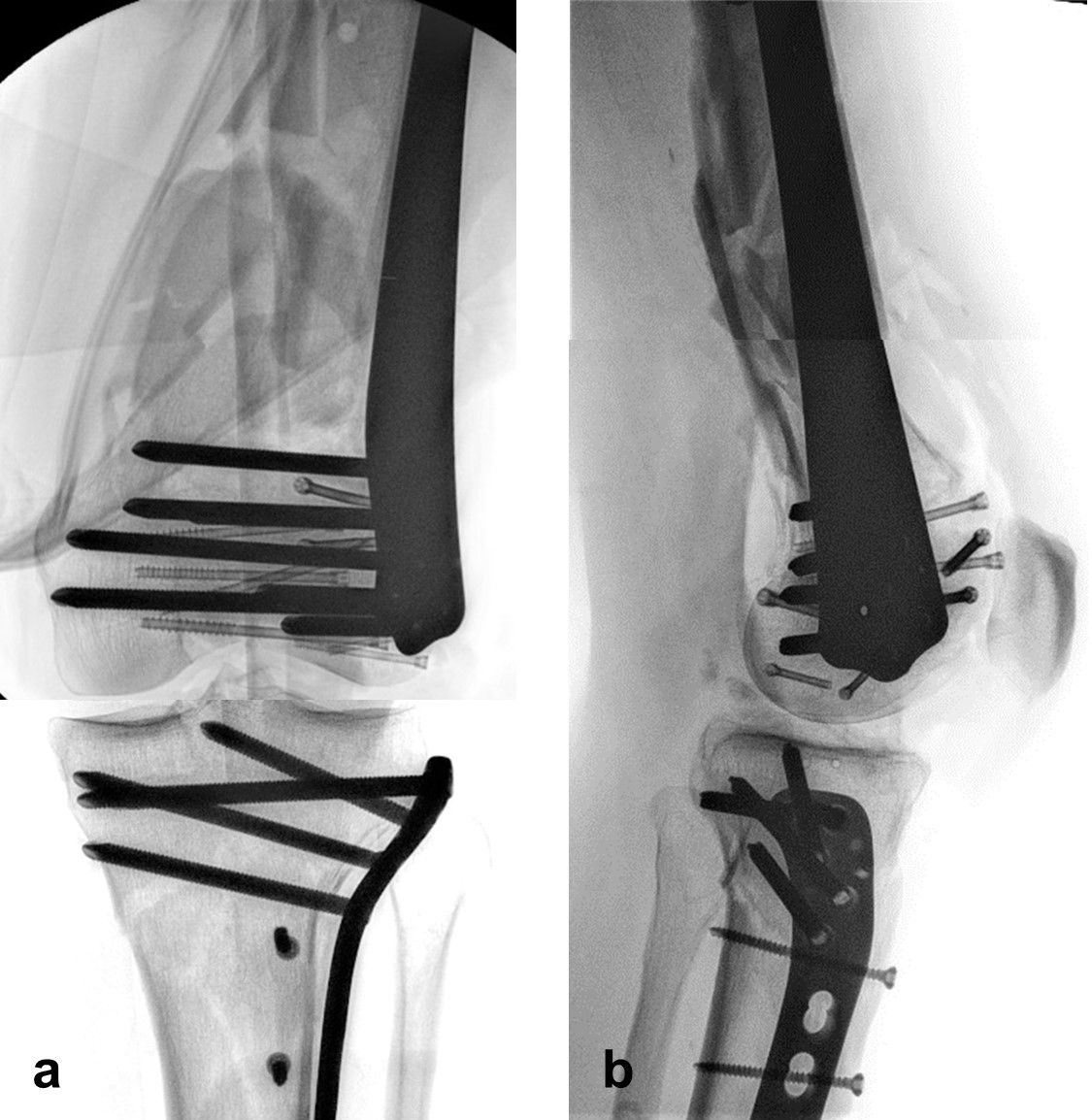 Fig 6a−b: AP (a) and ML (b) views after fixation with the Biphasic Plate DF.
Fig 6a−b: AP (a) and ML (b) views after fixation with the Biphasic Plate DF. 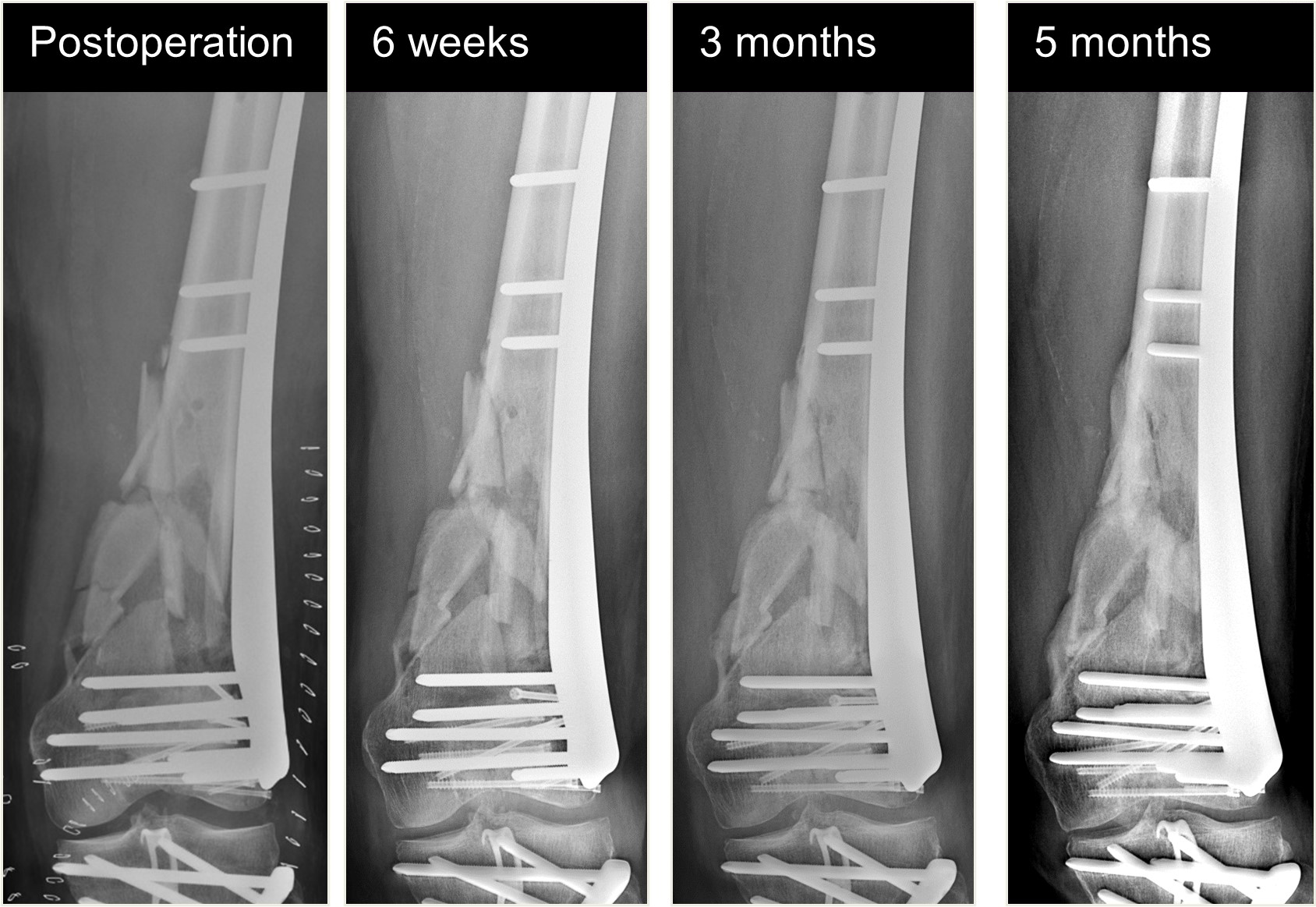 Fig 7: Healing progression is visible on AP radiographs over the course of 5 months.
Fig 7: Healing progression is visible on AP radiographs over the course of 5 months. Case 2
An 82-year-old man fell while climbing and sustained a periprosthetic distal femoral fracture (Fig 8). The fracture was reduced and then fixed with a Biphasic Plate DF (Fig 9). The patient was allowed immediate full weight bearing and presented with a decent amount of callus at the fracture site after 6 weeks (Fig 10).
The patient showed uneventful healing and returned to preoperative function 2.5 months postoperation. Figure 11 shows the callus formation 3 months postoperation.
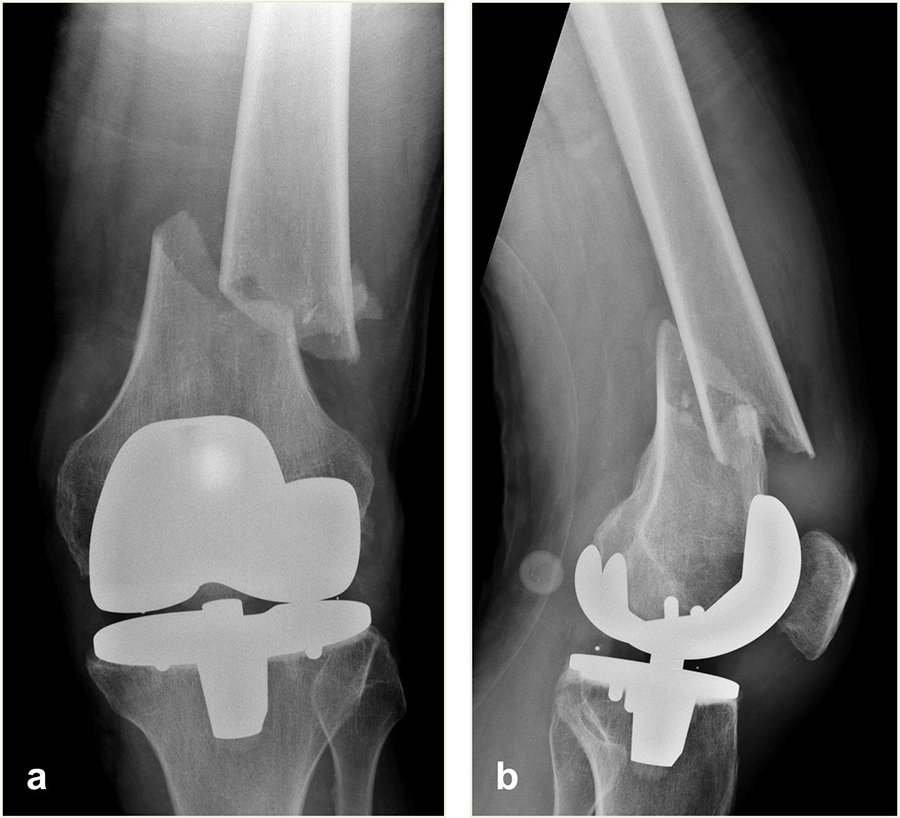 Fig 8a−b: AP (a) and ML (b) radiographs of the distal femoral fracture.
Fig 8a−b: AP (a) and ML (b) radiographs of the distal femoral fracture.  Fig 9a−b: AP (a) and ML (b) views after fixation with the Biphasic Plate DF.
Fig 9a−b: AP (a) and ML (b) views after fixation with the Biphasic Plate DF.  Fig 10a−b: AP (a) and ML (b) radiographs showing the formation of callus at 6 weeks postoperation.
Fig 10a−b: AP (a) and ML (b) radiographs showing the formation of callus at 6 weeks postoperation.  Fig 11a−b: AP (a) and ML (b) radiographs showing the formation of callus at 3 months postoperation.
Fig 11a−b: AP (a) and ML (b) radiographs showing the formation of callus at 3 months postoperation. Hazards and labeling
Due to varying countries’ legal and regulatory approval requirements, consult the appropriate local product labeling for approved intended use of the products described on this website. All devices on this website are approved by the AO Technical Commission. For logistical reasons, these devices may not be available in all countries worldwide at the date of publication.
Legal restrictions
This work was produced by AO Foundation, Switzerland. All rights reserved by AO Foundation. This publication, including all parts thereof, is legally protected by copyright.
Any use, exploitation or commercialization outside the narrow limits set forth by copyright legislation and the restrictions on use laid out below, without the publisher‘s consent, is illegal and liable to prosecution. This applies in particular to photostat reproduction, copying, scanning or duplication of any kind, translation, preparation of microfilms, electronic data processing, and storage such as making this publication available on Intranet or Internet.
Some of the products, names, instruments, treatments, logos, designs, etc referred to in this publication are also protected by patents, trademarks or by other intellectual property protection laws (eg, “AO” and the AO logo are subject to trademark applications/registrations) even though specific reference to this fact is not always made in the text. Therefore, the appearance of a name, instrument, etc without designation as proprietary is not to be construed as a representation by the publisher that it is in the public domain.
Restrictions on use: The rightful owner of an authorized copy of this work may use it for educational and research purposes only. Single images or illustrations may be copied for research or educational purposes only. The images or illustrations may not be altered in any way and need to carry the following statement of origin “Copyright by AO Foundation, Switzerland”.
Check www.aofoundation.org/disclaimer for more information.
If you have any comments or questions on the articles or the new devices, please do not hesitate to contact us.
“approved by AO Technical Commission” and “approved by AO Foundation”
The brands and labels “approved by AO Technical Commission” and “approved by AO Foundation”, particularly "AO" and the AO logo, are AO Foundation's intellectual property and subject to trademark applications and registrations, respectively. The use of these brands and labels is regulated by licensing agreements between AO Foundation and the producers of innovation products obliged to use such labels to declare the products as AO Technical Commission or AO Foundation approved solutions. Any unauthorized or inadequate use of these trademarks may be subject to legal action.

AO ITC Innovations Magazine
Find all issues of the AO ITC Innovations Magazine for download here.


Innovation Awards
Recognizing outstanding achievements in development and fostering excellence in surgical innovation.